CASE REPORT
Carotid web: an important cause of stroke in young people
Waite S,1 Nortley M,1 Howard DPJ,1 Flossmann E,2 Ford G2
Case report
A 40-year-old female presented 3 hours and 15 minutes after acute onset speech disturbance, left-sided weakness, headache and neck discomfort. She was a smoker and had a history of fibromyalgia and anxiety disorder. Her regular medications included a selective serotonin reuptake inhibitor and propranolol. Physical examination showed mild dysphasia and dysarthria, left hemiparesis (face, arm and leg) and sensory deficit with tactile neglect (National Institutes of Health Stroke Scale score of 7).
Computed tomography (CT) of the brain and angiography (CTA) of the neck vessels confirmed an evolving right middle cerebral artery (MCA) territory infarct and acute occlusion of the right MCA (M2). Thrombolysis was deemed futile, and she was started on aspirin 300 mg.
Furthermore, the CTA showed a ‘flap-like projection into the lumen of the right internal carotid artery (ICA)’ suggestive of a carotid web (Figure 1, arrow).
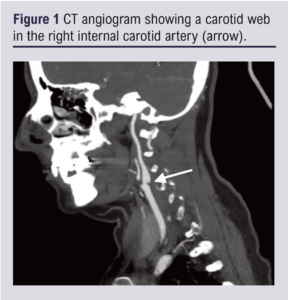
No defect was seen on cross-sectional views. Subsequent magnetic resonance angiography revealed ‘high signal at the posterior wall of the proximal right ICA’.
The patient was discharged on aspirin 75 mg. She made an excellent functional recovery and was re-imaged with CTA and duplex ultrasound at 4 months. CTA appearances of the ICA were unchanged. Duplex ultrasound showed no structural abnormality (Figure 2A) or significant flow disturbance (Figure 2B).
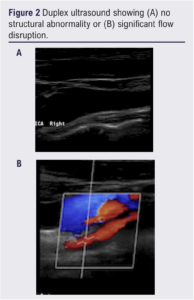
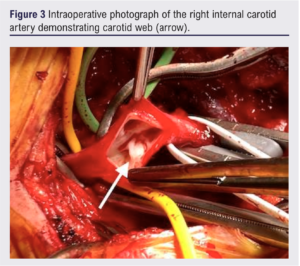
Peak systolic velocity within the ICA was 49 cm/s. Multidisciplinary team review recommended carotid endarterectomy because of a substantial risk of recurrent stroke. The web was removed surgically (Figure 3, arrow) and the ICA closed with a patch.1
Discussion
Carotid web is an increasingly recognised cause of stroke in young patients.2 It is a non-atherosclerotic fibromuscular dysplasia most commonly seen on the posterior wall of the origin of the ICA. It can be mistaken as carotid dissection and might not be apparent on some imaging modalities, particularly duplex ultrasound; CTA and digital subtraction angiography have good sensitivity.3 It is associated with a high risk of recurrent thrombo-embolism despite optimal medical therapy, even if the degree of stenosis is <50%. Stroke recurrence is rare after surgery or carotid stenting.4 A recent systematic review (37 articles, 158 patients) demonstrated the symptomatic carotid web population to have a high prevalence of women (68%) and African race (70%).4 The severity of stenosis caused by the carotid web was <50% in 84% of cases. Recurrent stroke was seen in 25 of 45 patients (56%) managed with antiplatelets or anticoagulants at a median time of 12 months. In 70 patients who underwent carotid revascularisation (50% carotid endarterectomy, 50% carotid artery stenting), no procedural complications were reported and recurrent stroke is rare.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2022;2(1):49-50
Publication date:
November 21, 2022
Author Affiliations:
1. Department of Vascular Surgery,
John Radcliffe Hospital, Oxford, UK
2. John Radcliffe Hospital, Oxford, UK
Corresponding author:
Seren Waite
Department of Vascular Surgery,
John Radcliffe Hospital, Oxford,
OX3 9DU, UK
Email: [email protected]


")

")

