ORIGINAL RESEARCH
Research priorities for vascular services: results of the UK Vascular James Lind Alliance Priority Setting Process
Long J,1,2 Gronlund T,3 Michaels J,4 on behalf of the Vascular Society of Great Britain and Ireland Service Special Interest Group
Plain English Summary
Why we undertook the work: More research is needed to help improve treatment and delivery of care for people with vascular conditions, but funding is limited. The Vascular Society of Great Britain and Ireland (VSGBI) ran a Priority Setting Process (PSP) to find out the most important research priorities. This helps researchers to better focus their work and helps funders to direct their support to projects that aim to answer questions that are important to people with lived experience and vascular health professionals. This paper presents the results of this process, focusing on vascular service related research priorities.
What we did: We asked vascular patients and healthcare professionals in separate surveys to suggest their own priorities for vascular research. Responses were summarised and organised into nine overall vascular condition areas, including a general ‘service’ category that incorporated issues relating to the organisation and delivery of services or cross-cutting themes. A summary list of questions was sent out and participants were asked to score them according to their importance. The lists of patient and professional priorities were then combined into a shared list for discussion at a final workshop meeting where a mix of patients and healthcare professionals agreed the ‘top 10’ research priorities for vascular services research in the UK.
What we found: A total of 481 healthcare professionals and 373 patients or carers submitted research priorities about vascular conditions, which were consolidated into a final combined list of 18 general priorities about vascular services. At a final workshop involving patients, carers and clinicians, these priorities were put into a ‘top 10’ list ranked according to perceived importance. Research priorities relate to: providing an efficient and fair service for vascular patients, education and training of clinicians and patients, improving communication and the introduction of new and better vascular treatments.
What this means: Research priorities considered most important for people with lived experience and vascular health professionals for vascular services have been identified. Researchers and funders are encouraged to focus on addressing these priorities and supporting studies in these areas.
Abstract
Introduction: The configuration of vascular services is a challenging process where treatment options, access and delivery of services is variable. There is a significant financial burden to the NHS due to rising demand for vascular services; however, guidelines for treatment options and delivery are frequently based on low levels of clinical and cost effectiveness evidence. Therefore, further research is required but capacity is limited and funding is highly competitive. To address this issue, the Vascular Society of Great Britain and Ireland (VSGBI) in association with the James Lind Alliance (JLA) undertook a national Priority Setting Process (PSP) for vascular conditions. This paper presents the results of this process, with a focus on the topic of ‘vascular services’.
Methods: A modified JLA Priority Setting Partnership was implemented in three overarching phases: (1) a clinician-led survey to gather clinician research priorities; (2) a patient and carer-led survey to gather patient and carer research priorities; (3) a consensus workshop to discuss clinician and patient priorities and agree a list of joint research priorities. Consensus was achieved using the nominal group technique and a ranked ‘top 10’ list of research priorities for vascular services was established.
Results: In the first phase (clinician-led survey), 481 clinicians submitted 1,231 research priorities related to vascular conditions in general. Of these, 338 service-related research priorities were reduced to 16 overarching summary priorities recirculated for interim scoring. In the second phase (patient and carer-led survey), 373 patients and carers submitted 582 research priorities. Of these, 25 service-related priorities were developed and recirculated for interim scoring. In the third phase (consensus workshop), clinician and patient priorities were amalgamated into 18 priorities for discussion. The final ‘top 10’ list of vascular service research priorities relate to: service configuration (organisation, access and delivery), patient experience, education and training (staff and patients), lifestyle and prevention, audit and evaluation and outcomes, diagnostics screening and risk assessment and communication.
Conclusion: The ‘top 10’ vascular service-related priorities demonstrate the research areas considered to be most important from the perspective of patients, carers and healthcare professionals. Researchers can now focus their efforts on addressing these important questions and funders should increase their investment to support new research in these areas of greatest importance.
Background
Vascular disease covers a broad spectrum of conditions and treatments, with over 40,000 vascular surgical procedures performed in England each year.1 It is one of the largest contributors to morbidity and mortality globally, accounting for 40% of deaths in the UK and estimated heath and care costs of £9 billion annually.2
Work conducted under the NHS Improvement programme Getting It Right First Time (GIRFT) and an NIHR Programme Grant for Applied Research (PGfAR) looking at configuration of vascular services both highlight considerable change in provision due to new treatment methods and increased specialisation.3,4 This has led to inconsistencies and local variation in practice, demonstrating the need for reorganisation of services to help address the challenges of increasing demand and rising treatment costs.
Research is fundamental in addressing these healthcare challenges. It underpins evidence-based practice and helps to inform how treatments and services are delivered. However, funding is limited and highly competitive, in particular the vascular specialty receives relatively little research investment compared with other specialties.5 Funding bodies need to ensure their limited investment is directed to areas with the greatest potential for improving clinical services and health outcomes whilst avoiding research waste.6 Significant investment in vascular research is needed to improve treatment and care.
Priority Setting Processes (PSPs) are an increasingly popular methodology to address this issue; they systematically identify and prioritise research gaps and are seen as an effective way of highlighting important topics for funding consideration.7 The Vascular Society of Great Britain and Ireland (VSGBI) initiated a national PSP for vascular conditions in association with the James Lind Alliance (JLA) who specialise in facilitating patient involvement in research.8 Prior to this, there was no agreement for research priorities within the vascular specialist community.
The aim of the Vascular PSP was to survey vascular health professionals, patients and carers to identify and generate a ranked list of the most important research priorities. This paper presents an overview of the vascular condition PSP, focusing on the recommendations for service-related priorities and implications for future research in this area.
Methods
A detailed description of the process has been provided previously,9-15 but is outlined again as a useful reference below and presented in Figure 1.

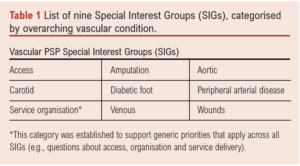
The VSGBI undertook a research PSP in association with the JLA to identify research priorities for vascular conditions. The work was overseen by a steering committee involving representation from all the leading UK Vascular Societies and patients. Nine overarching vascular condition Special Interest Groups (SIGs) were established to help support the process and ensure that each area retained their important research priorities (Table 1).
Initially, due to resource limitations, a clinician-led Delphi survey was conducted to produce a list of research priorities to reflect the opinions of vascular healthcare professionals. This was followed by a separate patient and carer focused JLA survey to identify important research priorities from the perspective of vascular patients and carers. The two processes were then brought together at final workshops held separately for each SIG, where patients, carers and clinicians worked together to agree a shared, ranked ‘top 10’ list of research priorities.
Scope of the Service SIG
Unlike the other vascular SIGs that are guided by a condition, the vascular service SIG was introduced to encompass the many submitted priorities that were considered general in scope and cross-cutting regardless of a particular vascular condition. The remit of the Service SIG is to support research into areas such as access, organisation and delivery of vascular services. The Service SIG aims to develop the list of top 10 priorities into funded research studies that address these important areas.
Clinician-led research Priority Setting Process
Healthcare professionals were surveyed using a modified Delphi approach that consisted of:
Survey Round One: In the first round, an open-ended survey invited participants to submit their priorities for vascular research. An electronic link to the survey was emailed via the following membership bodies: The Vascular Society of Great Britain, The Society of Vascular Nurses and The Society of Vascular Technicians of Great Britain and Ireland and the Rouleaux Club. Letters including the survey link were sent to each vascular unit registered on the National Vascular Registry (NVR) and the survey was also promoted via Twitter. Responses were collated and categorised into pathological topics and research themes by a core subgroup of the steering committee. Similar responses were amalgamated and summarised into an overarching priority. Responses considered out of scope (eg, too broad or logically unclear) were removed and remaining priorities checked for current evidence.
Survey Round Two: The refined list of priorities were redistributed in a second survey for scoring. Participants were asked to rate the importance of the summary priorities on a scale of 1–10 (1 being the least important, 10 being the most important). This process was completed in 201811 and the results of clinicians’ service-related priorities are summarised in Table 2.

Patient/carer-led research Priority Setting Process
Vascular patients and carers were surveyed using a modified JLA approach with guidance from a JLA advisor and using similar methodology to the clinician-led PSP.
Survey Round One: In the first round, patients and carers were invited to take part in an open-ended survey which asked them to submit their own research priorities. The survey was provided in paper and electronic format and advertised to UK-based societies involved with care of vascular patients. Participant packs were sent out to vascular units and included paper surveys with a freepost return address and promotional materials such as posters and postcards that could be left in waiting areas. The survey was also advertised via social media (Twitter), websites and newsletters. Responses were categorised and delegated to each SIG for further review. Similar responses were amalgamated and summarised into an overarching priority. Responses considered out of scope (eg, too broad or logically unclear) were removed and remaining responses checked for current evidence.
Survey Round Two: The refined list of priorities was redistributed in a second survey for scoring. Participants were invited to rate the importance of research priority using a Likert scale ranging from 1 = ‘not at all important’ to 5 = ‘extremely important’. This process was completed in 2020 and the results of patient and carer service-related priorities are summarised in Table 3.

Special Interest Group Prioritisation Workshops
For each SIG, the results of the clinician and patient/carer-led interim prioritisation processes were combined. Similar or duplicated priorities were amalgamated and any technically worded language from the clinician priorities was revised with patient input. Care was taken to ensure that the original substance of the priority remained. This process generated a refined list of joint priorities for discussion at individual SIG workshops.
The final prioritisation workshop for vascular services was conducted virtually on 9 July 2021 using the Zoom platform to accommodate COVID-19 restrictions. All attendees (including healthcare professionals, patients and carers) were recruited via direct contact or were approached if they expressed an interest during the initial prioritisation process. Participants were sent details of the workshop, an agenda and a list of the research priorities to be discussed in advance. Prior to the workshop, participants were asked to consider the combined list of clinician and patient research priorities shown in Table 4, and to rank them in order of importance from 1 (most important) to 18 (least important).

The workshop was led by two experienced JLA advisers, a JLA coordinator and a technical lead who were skilled in the JLA PSP process and leading such workshops. Members of the service SIG attended as observers and to provide emotional support to attendees if required (they would join a separate breakout room). SIG members were not directly involved in the priority setting and had no influence over the final agreed list of priorities. Following welcome and introductions, participants were split into three breakout rooms which consisted of a mix of patients, carers, clinicians and healthcare professionals. Small group discussions were facilitated by an advisor and followed a nominal group technique to reach a consensus for an ordered list of ‘top 10’ priorities.
First round of discussion: Participants shared their top three and lowest three priorities with a brief explanation for why. This was followed by an open discussion about similarities and differences and any priorities that were not initially mentioned.
Second round of discussion: The JLA facilitator presented on screen a potential order of questions based on initial feedback and discussion. Participants had an opportunity to reconsider their initial placement of priorities whilst the facilitator moved priorities on screen, to reflect an agreed order of priorities 1–18.
Third round of discussion: The ranked priorities of the separate groups were combined by the lead facilitator using a geometric mean of the respective ranked positions. All participants came together as one group and the lead facilitator presented the combined results of the group rankings. Participants were then split into new groups and, again, participants had an opportunity to reconsider the order of priorities before reaching a final ranked ‘top 10’ list of service research priorities. As before, the ranked priorities of the separate groups were combined to form a final shared ranking.
Results
Clinician research priority identification and prioritisation
A total of 481 clinicians submitted 1,231 research priorities relating to vascular conditions in general. Over 250 general service-related research priorities were submitted, 80 of which were excluded outright as they were too specific to single patient experience or there was no apparent question (eg, nonsensical or broad statement). The remaining priorities were combined and summarised into 16 clinician priorities for scoring, the results of which are shown in Table 2.
Patient/carer research priority identification and prioritisation
A total of 373 patients/carers suggested 582 research priorities related to vascular conditions in general, of which 73 responses were directly assigned to the Service SIG, together with a further 96 cross-cutting responses shared from other SIG categories. After data cleaning (eg, removing nonsensical suggestions, separating out submissions with multiple suggestions and combining overlapping priorities), 18 summary research priorities were developed. An additional seven summary priorities were suggested based upon SIG review of published research and SIG members’ knowledge of gaps in this area not addressed by submitted responses. A total of 25 summary priorities were redistributed for scoring and the results are shown in Table 3. Prior to the workshop, the SIG team pooled clinician and patient/carer research priorities, resulting in a list of 18 for discussion (Table 4). In order to reduce risk of bias, these priorities were randomly ordered and each assigned a letter (rather than a number).
Final prioritisation workshop
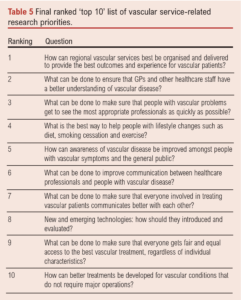
The final prioritisation process was conducted via a virtual online meeting on 9 July 2021. It was attended by nine patients and carers with experience of a range of vascular conditions and nine healthcare professionals representing vascular nurses, vascular surgeons, vascular scientists, podiatrists and public health representatives, plus five observers. The final prioritisation resulted in a final ‘top 10’ research priority list (Table 5). The priorities are ordered according to importance as determined at the workshop. There was general consensus that the list correctly represented the discussions and viewpoints which occurred in the breakout groups. Results from participant feedback indicated that over 80% agreed or strongly agreed that the process of determining the ‘top 10’ was robust and fair.
Discussion
The ‘top 10’ research priorities for UK vascular service research have now been established. Using a modified JLA methodology, vascular healthcare professionals and patients with lived experience of vascular conditions have jointly agreed the most important priorities for future research in this area.
Overarching themes within the final top 10 list relate to service configuration, patient experience, education and training, lifestyle and prevention, audit, evaluation and outcomes, diagnostics screening and risk assessment and communication. Priorities 1, 3 and 9 focus on access to services and optimising service delivery. Priorities 2, 4 and 5 relate to education and training of clinicians and patients to raise awareness of conditions and referral processes. Priorities 6 and 7 appear similar but there was an important distinction in improving communication between patients and clinicians but also improving communication between clinicians. Priority 8 addresses the introduction and evaluation of new treatments.
The priorities dovetail well with the recommendations from the aforementioned NIHR PGfAR.4 The priorities not in the ranked ‘top 10’ list should still be considered important and merit further research.
Strengths and limitations
Strengths and limitations of the vascular PSP process have already been documented in previous publications of SIG results but are provided again here with additional reference to the Service SIG workshop feedback.
The Vascular PSP used well established methodologies throughout, with oversight from a multidisciplinary steering committee. The Delphi method, often used in priority setting processes, is regarded as a flexible research technique but one that tends to focus on the identification of expert opinion.16 To mitigate this, the Vascular PSP sought the input of the JLA who provide a transparent and structured framework that emphasises patient participation in PSPs, with patients having an equal voice to clinicians and researchers in influencing the research agenda.17,18 It is possible that the modified approach of having two separate processes before bringing the clinician and patient views together may have resulted in a different ‘top 10’. However, during the amalgamation process there were significant similarities between clinician and patient priorities and the format of the final workshops established valid shared priorities.
The survey data collection process potentially predisposed to responder bias.19 Consideration was given to whether responses would adequately reflect the opinions of people with lived experience of vascular conditions and those treating them. Under-representation is a well-documented limitation of many PSPs,20,21 with the associated potential implication that other relevant priorities may not be submitted or considered. The Vascular PSP sought to minimise this risk in a number of ways. The survey was made available in electronic and hardcopy format (with freepost address), and it was promoted via a number of platforms with the help of affiliated charity groups and organisations who regularly work with the targeted population. Furthermore, the introduction of SIGs meant that each vascular condition area had a dedicated review of responses by a group of interested professionals and patients who could highlight expected topic areas that were absent or under-represented.
Most workshop participants found the use of a virtual platform acceptable, but one participant from the Service SIG workshop suggested that it should have been held over a whole day to allow more time for discussion. Potentially, lack of access to IT may have limited participation and altered representation; however, the virtual platform meant patients did not have to travel, and this may have made the workshop more accessible for some patients.
Positive comments collected from the feedback survey following the final workshop demonstrated that clinicians and patients found the process of discussing priorities in mixed groups a positive and worthwhile experience. It gave participants an opportunity to consider other peoples’ experiences and reassess their initial judgements.22 One participant feedback commented, “It was very interesting debating with the medical professionals, whose original priorities were almost at the other end of the list to mine”.
The mixed discussion groups were carefully moderated through the skilled JLA facilitators who ensured that patient participants were regularly included and asked for their views. Some participants expressed a preference for a different ranking order of the priorities, but this is not uncommon for PSPs and is a known factor of a consensus approach.
This particular SIG raised some specific issues in the priority setting exercise. Obtaining adequate patient/carer representation is an important part of the process, but the online questionnaire focused on diagnosis and treatment of specific conditions, and it is likely that individual patients/carers will have experience of vascular services that are limited to a particular condition and local service providers. Thus, questions that relate to the wider configuration of services and variation in practice may not be within the participants’ experience. There were also a number of themes that were raised in relation to specific conditions and/or as general topics, particularly issues related to communication, referral processes and access to services.
Implications for future research
The Service SIG priorities now provide researchers with essential guidance on where best to focus their efforts in the immediate and long term. Due to the broad encompassing nature of the Service SIG, it will benefit from wider input from each of the SIGs to help develop projects to address these important priorities. We call on funders to recognise and support the delivery of this important work.
Conclusion
The Vascular PSP has established a ‘top 10’ list of priorities for UK vascular service research from the shared perspective of vascular patients, carers and health professionals. Researchers and funders can confidently invest resources into these areas of vascular service research with reassurance that they are clinically relevant and of utmost practical importance to patients.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2022;2(1):33-40
Publication date:
November 21, 2022
Author Affiliations:
1. Hull University Teaching Hospitals NHS Trust, Hull, UK
2. Academic Vascular Surgical Unit, Hull York Medical School, Hull, UK
3. James Lind Alliance, UK
4. School of Health and Related Research, The University of Sheffield, Sheffield, UK
Corresponding author:
Judith Long
Vascular Office, 2nd Floor,
Allam Diabetes Centre,
Hull Royal Infirmary,
Anlaby Road, Hull, HU3 2JZ, UK
Email: [email protected]


")

")

