EDITORIALS
Vascular Surgery Curriculum 2021: the trainee perspective
Nickinson ATO,1,2 Travers HC3,4
The 2021 iteration of the Vascular Surgery Curriculum represents the first major change to vascular training since being awarded separate specialty status by the General Medical Council (GMC) in 2013.1 Developed following the ‘Shape of Training’ review and in light of updated GMC guidance on postgraduate curricula, the new curriculum aims to specify the professional standards and clinical capabilities required to provide trainees with the competencies to be a day 1 consultant vascular surgeon in modern clinical practice.2,3 The process of transition started in August 2021, with all trainees migrating to the new curriculum by August 2023. From a trainee perspective, the new curriculum offers a number of positive changes which should improve the process of working towards certification.
Focus on outcomes
Being a consultant vascular surgeon requires the integration of a broad array of clinical and professional skills across multiple clinical settings. Clearly, demonstrating proficiency in these skills as a trainee is more than just completing a defined number of workplace-based assessments (WBAs) or a set number of training years.
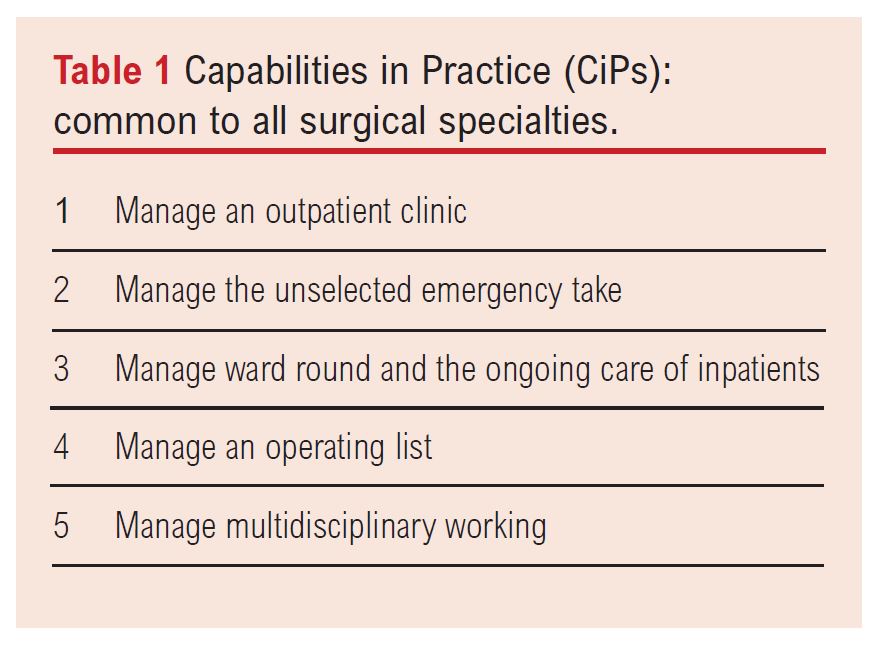
One welcome area of major change is the shift in focus towards outcomes, based around the expectation of what is required to competently perform as a day 1 consultant. Set around the concepts of ‘Capabilities in Practice’ (CiPs) and ‘Generic Professional Capabilities’ (GPCs), trainees will be required to demonstrate generic and specific vascular competencies across all areas of work (Table 1), from managing an operating list to multidisciplinary team working. Defining outcomes in this way provides trainees with a more ‘real-world’ understanding of the requirements for certification and provides greater context to the training syllabus. For the first time, the curriculum also defines and recognises excellence in training for those trainees exceeding expectations – a welcome addition.
The new curriculum also affords greater flexibility for trainees, particularly in terms of the length of training; the indicative six years can be shortened (or lengthened), based upon the rate of progression. This brings equality amongst all trainees. Historically, those in academic training who worked part time in clinical practice did not automatically have their training time lengthened; however, those in less than full time training for any other reason automatically had their training extended pro rata, irrespective of competence. Trainees moving into vascular surgery from other specialities can also transfer generic competencies to count towards training, something which to date has been highly challenging to define.
The Multiple Consultant Report
Arguably the biggest change to the new curriculum is the introduction of the Multiple Consultant Report (MCR), which forms the primary assessment tool within the workplace. The MCR involves clinical supervisors meeting to discuss the supervision level reached by a trainee in each of the CiPs, in addition to providing judgement on the development of GPCs and identifying the short to medium term training needs to help a trainee progress towards certification. The information from this is then used by a trainee’s assigned educational supervisor in combination with other evidence (eg, WBAs) to provide the end of placement report, which feeds into the Annual Review of Competence Progression (ARCP) process. Feedback from the MCR, with points for development, also automatically feed into the trainees’ next learning agreement, focusing on areas where development is required. Although a major change, the MCR will hopefully provide a more accurate, up-to-date and complete judgement on a trainee’s progression, which focuses on all aspects of work.
Crucially, the MCR also helps to rebalance the role of WBAs. Traditionally, WBAs have been the cornerstone of training, providing evidence of competencies across all parts of the curriculum. When used correctly, they are an excellent tool for demonstrating learning and receiving feedback; however, the focus on completing a minimum number – rather than their quality – undoubtedly detracts from their usefulness as an assessment tool. Although WBAs will still be a tool to demonstrate competencies in the syllabus ‘critical conditions’ and ‘index procedures’, the introduction of the MCR removes the need to complete a minimum number per training year. This welcome change not only helps to improve the role of WBAs for trainees, but also reduces the burden on assessment on both trainees and trainers.
Clarity of trainee progression
Although having clarity on the expectations for certification is vital, as important is a clear expectation on the rate of progression, particularly for those in the middle years of training. Whilst under the previous curriculum benchmarking checklists were available, these primarily focused on operative experience and acted as simple ‘tick-box’ lists rather than giving a global appreciation of how trainees were progressing.
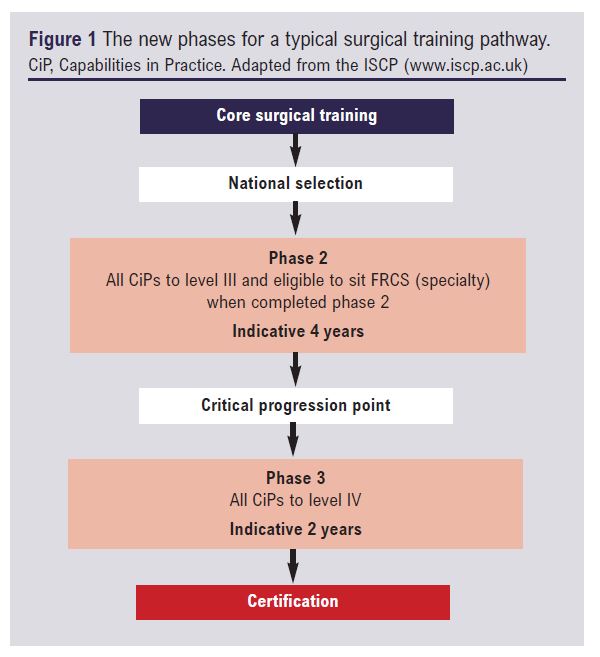
Within the 2021 curriculum, this changes with training being arranged into three distinct phases, extending from core surgical training to final certification (Figure 1). The junction between phases 2 (ST3-6) and 3 (ST7-8) now acts as a ‘critical progression point’, with progress based upon clearly defined requirements across all CiPs. For trainees, this not only provides greater clarity on their expected progression across all aspects of work, but also sets an objective benchmark for when trainees are deemed suitable to sit the Intercollegiate Specialty Examination in Vascular Surgery.
In addition to the benefits for trainees with a National Training Number (NTN), the new curriculum will hopefully provide greater clarity for those trainees applying for specialist registration through the Certificate of Eligibility for Specialist Registration (CESR) route, as mapping their competencies to CiPs, GCPs and index procedures, along with MCRs, will clearly demonstrate ‘equivalence’ with NTN trainees. This should help with the workforce crisis currently faced by vascular surgery in the UK.4
The proof of the pudding…
It is of course too early to make firm judgements about the success of these changes; however, with transition already in progress, many trainees should soon be getting first-hand experience of the new curriculum. Although it will undoubtedly take some time to adjust, credit must be given to the Intercollegiate Surgical Curriculum Programme (ISCP) for their clear advice and willingness to engage with trainees about the new process. Ultimately, the proof of the pudding is in the eating; however, at first look the new curriculum has the right ingredients to make a real positive change for trainees.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2022;1(2):21-22
Publication date:
February 21, 2022
Author Affiliations:
1.Vascular Surgery Specialty Registrar, University Hospitals of Southampton NHS Foundation Trust, Southampton, UK
2.Rouleaux Club Specialist Advisor Committee (SAC) Representative
3.Vascular Surgery Specialty Registrar, Birmingham Vascular Centre, University Hospitals of Birmingham NHS Foundation Trust, Birmingham, UK
4.Rouleaux Club Immediate Past President


")

")

