ORIGINAL RESEARCH
The prevalence and solutions to burnout amongst surgical trainees
Nasim A,1 Srinivasmurthy D,2 Searle H,2 Yu Y-Y1
Plain English Summary
Why we undertook the work: Burnout is characterised by the following three symptoms: (1) emotional exhaustion; (2) reduced sense of personal accomplishment; and (3) loss of sense of self. Burnout is increasingly affecting all healthcare workers in the UK. Surgical trainees, particularly female trainees, are dropping out at a higher rate. Burnout may be contributing to the surgical trainee drop-out rates. Unfortunately, there is not enough research on this topic. There is limited information on how to reduce burnout among surgical trainees. This review aims to report burnout rates among surgical trainees and find ways to reduce burnout and improve trainee well-being.
What we did: We systematically analysed the literature looking for papers which reported how common burnout is in surgical trainees, whether there was a difference in burnout between male and female trainees, and what interventions may reduce burnout.
What we found: We identified 22 relevant papers on burnout in surgical trainees, 11 of which focused on burnout rates among female and junior surgical trainees and the other 11 papers highlighted methods to help reduce burnout in surgical trainees and how to implement them. Trainees reporting prejudice, abuse or harassment are more likely to experience burnout, regardless of gender. There were conflicting results found on burnout prevalence and training level. Interventions identified to help combat burnout were mindfulness courses, mentorship programmes, stress resilience training and self-compassion training.
What this means: Female and junior trainees are more at risk of exposure to negative behaviours in the workplace. This contributes to higher levels of burnout. Mentorship, mindfulness and resilience training may reduce burnout and improve surgical trainee well-being, but more needs to be done to educate faculty and raise awareness amongst surgical peers.
Abstract
Background: Burnout is a syndrome of emotional exhaustion, reduced sense of personal accomplishment and loss of sense of self. Healthcare workers in the UK are known to suffer high psychological distress and burnout. Increasing attrition rates among surgical trainees have also been noted, particularly among female trainees. However, there are limited data on the factors contributing to burnout potentially leading to trainee attrition. Interventions to combat burnout and improve trainee well-being are still in their infancy. This review reports burnout prevalence and methods implemented to reduce burnout and improve surgical trainee well-being.
Objective: To report the prevalence and factors contributing to burnout and suggest evidence-based methods that reduce burnout and improve well-being within this cohort.
Methods: A literature search was conducted across five databases, identifying papers on burnout prevalence among surgical trainees and reported gender. Papers outlining interventions to reduce burnout were also included. Papers were screened against our inclusion and exclusion criteria. Quality was assessed using the modified Newcastle–Ottawa Scale and data were extracted and presented in this review.
Results: Following screening, 22 of 456 identified papers were included in the review; 11 papers were examined for burnout prevalence and the remaining 11 papers focused on interventions. Trainees reporting discrimination, abuse or harassment at least once a month were significantly more likely to experience burnout regardless of gender. Conflicting results were found on burnout prevalence and training level. Interventions identified included mindfulness courses, mentorship programmes, Enhanced Stress Resilience Training (ESRT) and Self-Compassion for Healthcare Communities (SCHC) training. Dedicated faculty and wellness opportunities produced lower burnout rates (p=0.02). Two months of mindfulness training via the Headspace application also reduced burnout scores (p=0.01). ESRT reduced overall burnout by 38.9%. Similarly, increased self-compassion significantly predicted burnout reduction (p=0.018). No significant improvement was identified in residents at unionised programmes.
Conclusions: While there was no significant difference in burnout between genders, female and junior trainees are more at risk of exposure to negative behaviours in the workplace. This can directly contribute to higher levels of burnout. Interventions like mentorship and mindfulness and resilience training may reduce burnout and improve surgical trainee well-being. However, more needs to be done to educate faculty and raise awareness amongst surgical peers.
Introduction
Following the COVID-19 pandemic, healthcare workers in the UK suffer high psychological distress.1 Increasing attrition rates globally, especially among female surgical trainees, highlight the need for prioritising surgical trainee well-being.2–4 However, there are limited data on the mental well-being and burnout experienced by surgeons and surgical trainees.
Burnout is a syndrome comprising emotional exhaustion, depersonalisation and reduced sense of personal accomplishment.5 In 2021, 32% of UK surgeons reported burnout. Surgical trainees documented the highest average prevalence of 59% compared with 41% of consultants.6 Surgical trainees also reported an 83% incidence of mild psychiatric illness, 83% disengagement and 87% exhaustion.7 Poor mental well-being causes personal consequences such as higher levels of depression, anxiety, post-traumatic stress disorder (PTSD) and suicidal ideations, all affiliated with burnout. This leads to increased healthcare use and decreases functional status, debilitating trainees’ ability to work.8,9
Despite limited research on patient outcomes, those reporting burnout have a higher self-reported risk of medical errors resulting in harm. The same was reported for near-misses not resulting in harm.8,10 Similarly, surgical trainees reporting burnout were more likely to shout at their patients and make medical errors.11-13
Factors such as age, marital status, children, work-life balance and mental health are known to contribute to burnout.14,15 In particular, female and junior surgical trainees have a higher risk of burnout.15 However, previous reviews have not focused solely on surgical trainees, particularly those at a junior level and female.16 Interventions for burnout and well-being are still in their infancy.17 This review aims to report the prevalence and factors contributing to burnout and suggest evidence-based methods that may improve burnout and well-being within this cohort.
Research questions
• What is the prevalence of burnout among surgical trainees?
• Is prevalence affected by sex or training grade?
• What interventions are available to surgical trainees to combat burnout and improve well-being?
• What are the current gaps in research about improving burnout and well-being in surgical trainees?
Methods
The development of this scoping review was documented and conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Checklist.18
Inclusion and exclusion criteria
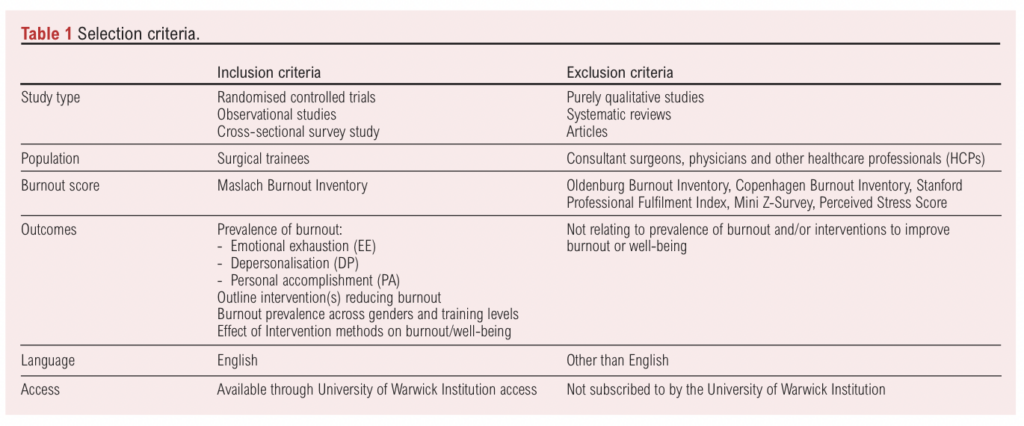
The inclusion and exclusion criteria are outlined in Table 1. Systematic reviews were excluded but separately examined to ensure all relevant studies were included. Studies included spanned the globe due to the lack of literature focusing on UK surgical training programmes. Well-being interventions were defined by the authors and were included if burnout outcomes were measured using the Maslach Burnout Inventory (MBI). Only studies recorded in the English language were included. No timeframe was specified in order to identify as many interventions as possible.
Outcome measures
The primary outcome measure was burnout using the MBI. MBI is the ‘gold-standard’ and most reliable measure for professionals working with others.19 Despite the MBI receiving criticism for discounting burnout in informal work environments, it is an appropriate choice for assessing burnout in a healthcare workplace and was therefore used in this study.
Maslach Burnout Inventory (MBI)
Standard MBI is a 22-item burnout assessment tool widely adopted by healthcare workers. It measures three dimensions: nine measure emotional exhaustion (EE), five evaluate depersonalisation (DP) and eight measure personal accomplishment (PA). Individuals scoring highly on EE and DP and scoring low on PA were associated with a high risk of burnout.19,20 Studies included in this review adopted variations of the MBI, including a two-item, nine-item and the full 22-item MBI.
Literature search strategy
Five databases (Medline, Embase, PsycInfo, Scopus and Web of Science) were electronically searched on 6 October 2023 for English language studies conducted prior to this date. Search strategies included text terms, MeSH terms and Boolean operators. Reference lists and citation searches were subsequently performed to identify sources not highlighted in these databases.
PROSPERO was also searched for existing and ongoing systematic reviews on burnout in surgical trainees. Two protocols were identified on surgeon burnout; however, their aims, inclusion and exclusion criteria differed from this review. One of the identified reviews focused on the effects of burnout on patient outcomes and surgical professionalism,21 while the other explored trends in burnout prevalence across Canada and America over time.22
Screening
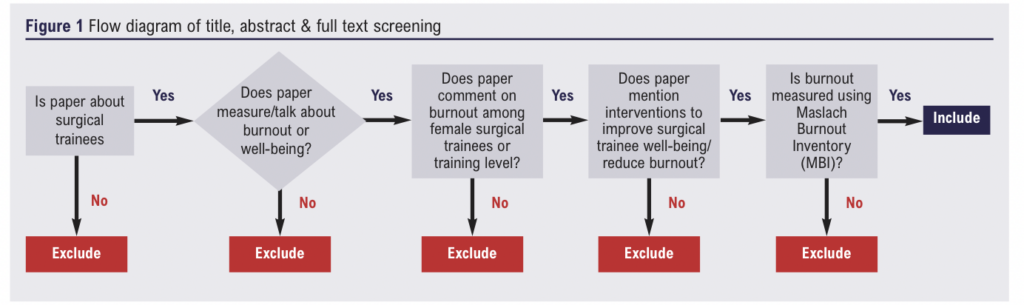
Two investigators (AN and YYY) independently screened titles, abstracts and full texts for inclusion with disagreements resolved through discussion. The same manual method was used for all screening (Figure 1).
Data extraction and synthesis
Data from the included studies were extracted as follows: author name, title, year of publication, during COVID-19 pandemic, location and type of study, sample size, number of male and female participants, diagnostic tool and burnout definition used, outcome measures, intervention performed, duration of data collection and results. Data were extracted independently on a spreadsheet by two investigators (AN and YYY) and any disparities were resolved through discussion.
Results
Search outcome
A systematic search produced 616 results from five databases, 160 of which were duplicates. Following duplicate removal, 362 of the remaining 456 studies were excluded following title and abstract suitability screening. Following full text screening of the remaining papers, 22 were considered eligible for inclusion in the analysis (Figure 2). Eleven papers were examined for burnout prevalence and the remaining 11 papers focused on interventions.
![]()
Quality assessment
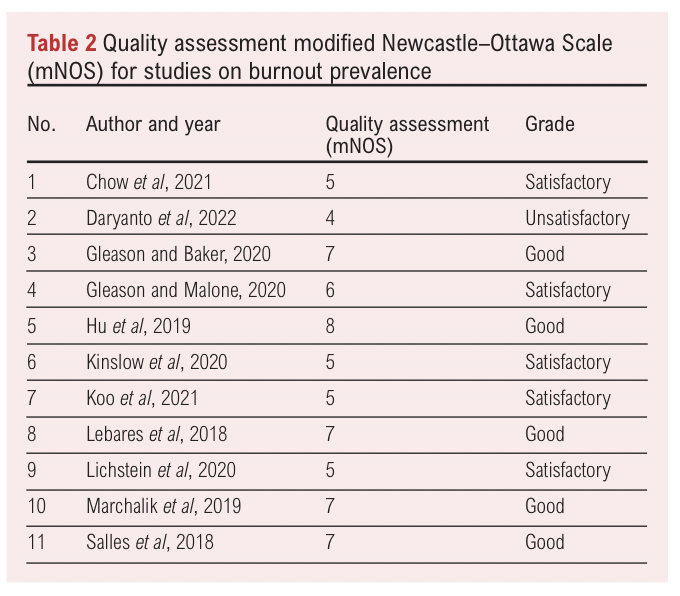
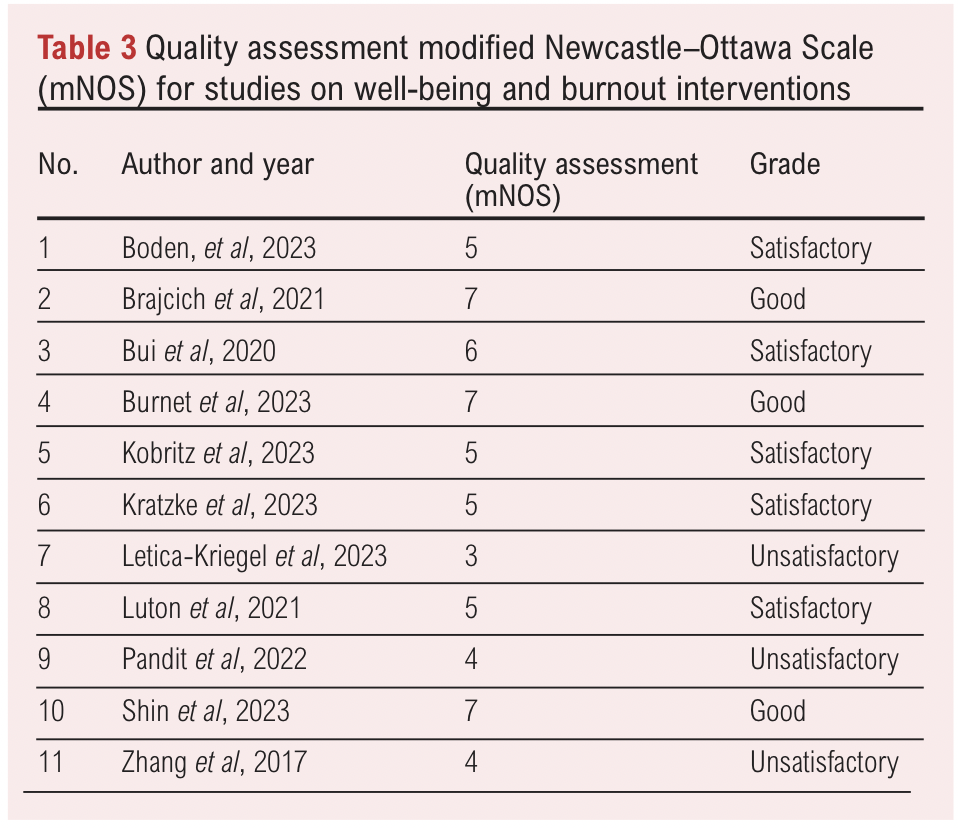
Quality was assessed by two independent reviewers (AN and YYY) using the modified Newcastle–Ottawa Scale (NOS) for cross-sectional studies. Discrepancies were resolved through discussion.23 Although meta-analytical pooling was planned, variation in study designs, burnout ascertainment methods and statistical heterogeneity made quantitative pooling inappropriate. Therefore, studies were summarised descriptively and assessed qualitatively (Tables 2 & 3).
Description of included studies
Table 4 summarises the sample and design of the included studies reporting prevalence of burnout among surgical trainees. All studies (N=11) reported sample sizes, ranging from 34 to 7409, and specified the gender of participants. Most studies (N=9) had a higher number of male participants, which may be due to the higher number of men currently in the surgical field. Participants’ training level ranged from 1 year post graduation to more senior levels at PGY level 4 and above.
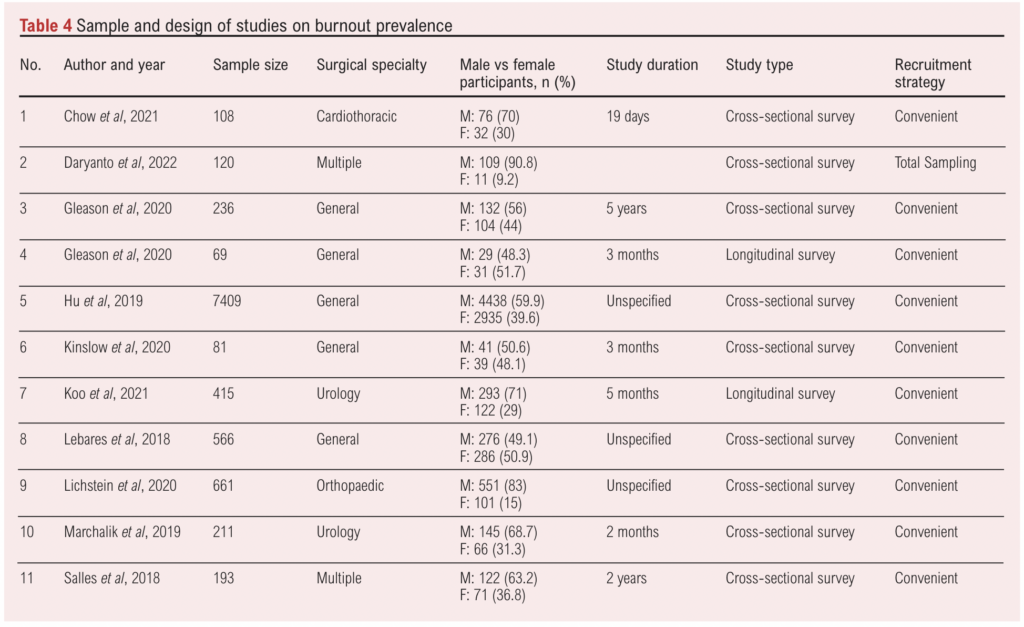
Only one study on burnout prevalence included in this review was conducted in Indonesia,24 the other 10 included studies originated in the USA.25-34 Due to the differences in location, surgical training programmes differed greatly, even across training programmes in the USA, therefore factors contributing to burnout may not be generalisable to other surgical training programmes.
Three studies did not state study duration.25,26,29 The other nine varied in timeframe, ranging from 19 days to 5 years.
Most studies (N=10) adopted a convenient sampling method. Only one used total sampling. Due to the volunteer-based participation, recruited participants were probably self-aware and motivated to engage, making it difficult to eliminate non-response and selection bias.
Prevalence of burnout among surgical trainees and contributing factors
Burnout based on gender
Nine papers investigated the relationship between sex and prevalence of burnout (Table 5).24-26,28-31,33,34 Of the nine studies, this was the primary outcome in six studies,25,26,28,30,33,34 while the other three explored this association as a secondary outcome.24,29,31 Female residents reportedly experience higher rates of burnout. However, this review found four papers highlighting workplace bullying and harassment as leading factors contributing to burnout, regardless of gender.25,28,31,33
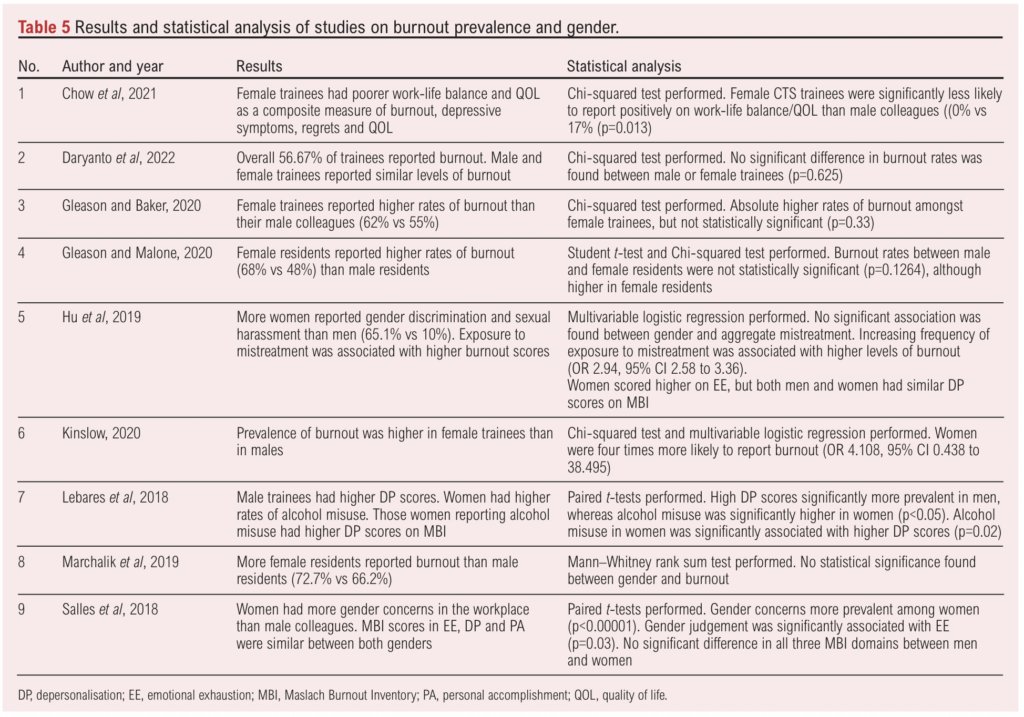
Female surgical trainees were more likely to experience mistreatment in the workplace than their male colleagues (65.1% reported gender discrimination, 30.3% reported sexual harassment). Trainees reporting discrimination, abuse or harassment at least once a month experienced burnout symptoms significantly more (OR 2.94; 95% CI 2.58 to 3.36).25
Similarly, Kinslow et al found that female trainees reported burnout 2.7 times more than men.30 Women also had more gender judgement concerns, which were significantly associated with higher burnout scores in all three MBI domains (p<0.013).28
In contrast, Lebares et al found higher DP among male residents.26 However, in the same study female trainees had higher rates of alcohol misuse, also associated with higher DP scores as well as low anxiety. The alcohol misuse may provide a falsely low burnout score among women, and highlights a negative coping mechanism.26 When accounting for burnout, depressive symptoms, quality of life (QOL) and work-life balance, female CTS trainees were significantly more likely to report negative balance/QOL outcomes (p=0.013). It was alluded that this may be due to the increased prevalence of mistreatment experienced by female trainees. However, their study did not identify any gender-related differences in burnout.31
Although women reported higher burnout rates in the other included studies, no significant difference was found in burnout prevalence between genders.24,29,31–34
Burnout based on training level
Seven studies reported burnout outcomes across surgical training levels (Table 6). Only two studies explored this relationship as a primary aim.
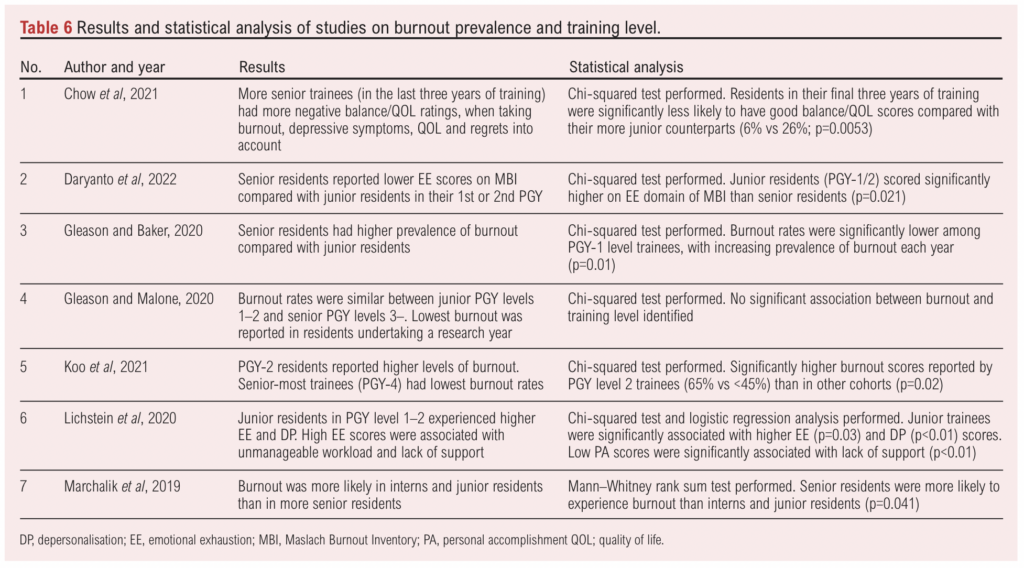
Conflicting results were observed. Four studies reported that junior residents experience more burnout,24,27,32,34 while two reported that senior residents experience more burnout.29,31 The remaining other study found no association between training level and burnout prevalence.33
72.9% of junior residents reported significantly higher DP scores than senior residents (60%) (p=0.041 and OR 1.27, 95% CI 1.12 to 1.41; p<0.01, respectively).27,34 However, the training level did not remain statistically significant on multivariable analysis.34 Similarly, PGY-1 residents reported higher levels of EE compared with senior level trainees (p=0.021 and (OR 1.15, 95% CI 1.01 to 1.32; p=0.03, respectively).24,27
Contrary to this, Gleason et al reported that PGY-1 level trainees had the lowest rates of burnout across training years. Burnout levels increased the further along training residents were, peaking in graduating residents (p=0.01).29 Chow et al reported similar findings, with trainees in the latter years of their CTS training reporting significantly increased burnout.31
Other studies found no association between training level and burnout. Instead, specific training years were identified as causing higher rates of burnout. For example, Koo et al reported that trainees in PGY-2 training had significantly higher burnout compared with other training years (p=0.02).32
Only one of the included studies reported no association between training level and prevalence of burnout.33
Identified interventions for burnout and well-being
Eleven studies exploring well-being and burnout interventions met the inclusion criteria (Table 7).35-45 Participants’ training level ranged from PGY level 1 to PGY level 4 and above. All papers specified surgical specialty. Four studies involved general surgery residents, one on otolaryngology residents, one on orthopaedic residents, one on neurosurgery residents and four on multiple surgical specialties.
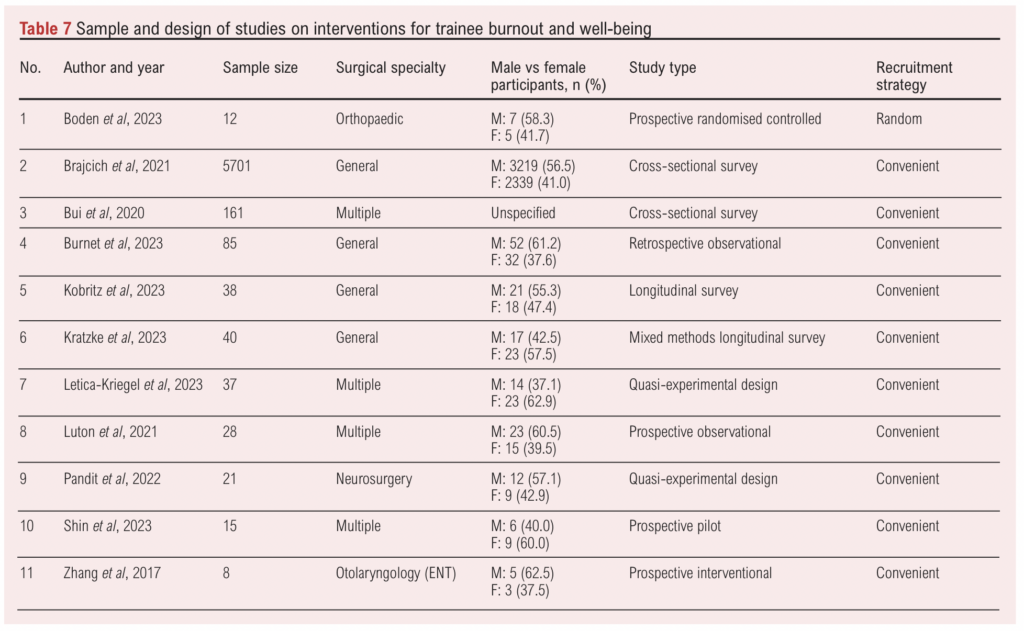
Two studies were pilot studies,40,45 two were cross-sectional studies35,36 and two were longitudinal studies.37,38 A further two opted for a quasi-experimental design.39,40 Of the three remaining prospective studies, one was a randomised controlled trial,40 one was an observational survey42 while the other was an interventional study.43
All studies reported their recruitment strategy, with the majority using convenient sampling.34–39,41–43,46 Only one opted for random sampling with a control.40
Sample sizes varied across studies, ranging from eight to 5,701 participants. All studies stated participants’ gender except one.36 Only three studies had a larger proportion of female participants.38,39,45
The volunteer-based nature of participant recruitment meant selection and non-response bias was present. Findings could not be generalised to the wider surgical trainee population as participants were self-motivated and self-aware. Participants experiencing burnout symptoms may have been either more or less likely to participate, contributing to response bias.
Study duration ranged between 4 weeks and a year. Studies from across the globe were included with seven studies from the USA,35–39,41,46 two from the UK,40,42 and one each from Canada and South Korea, respectively.43,45
Interventions performed and analysis
Table 8 outlines interventions from the included studies. Interventions varied significantly and consisted of mindfulness courses,36,39–41,44 mentorship programmes,37,43 Enhanced Stress Resilience Training (ESRT)42 and Self-Compassion for Healthcare Communities (SCHC) training.38,45
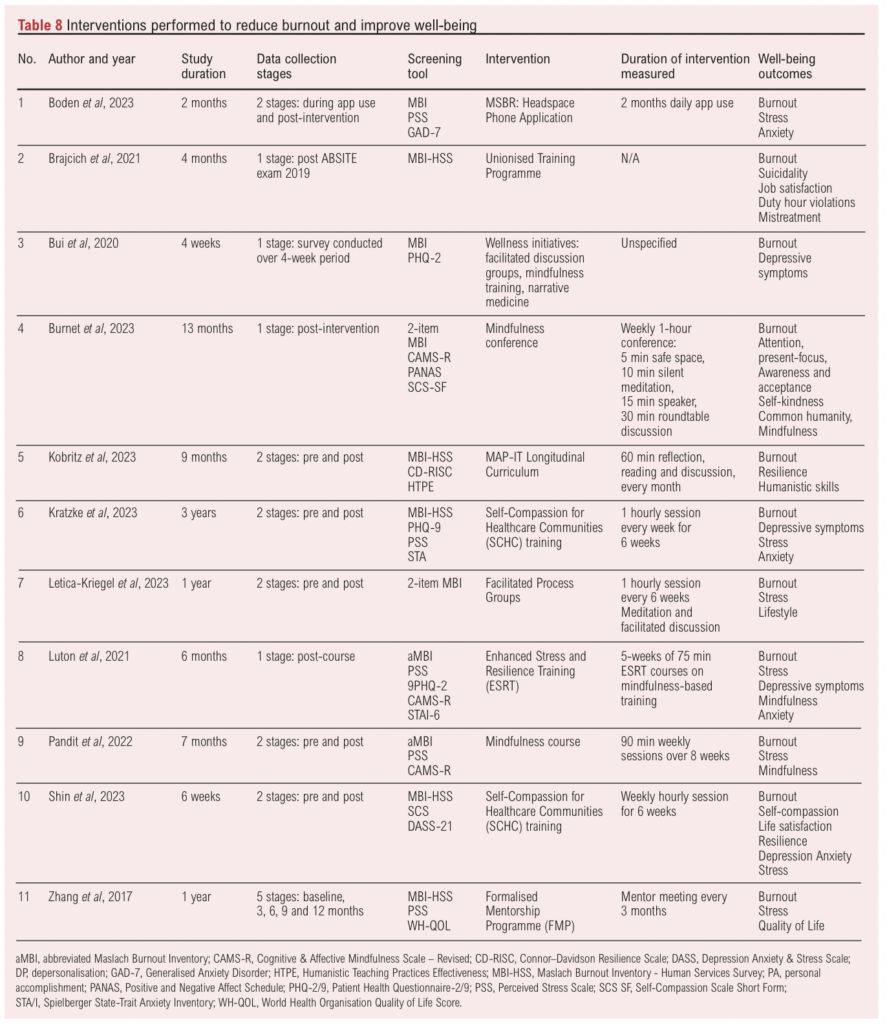
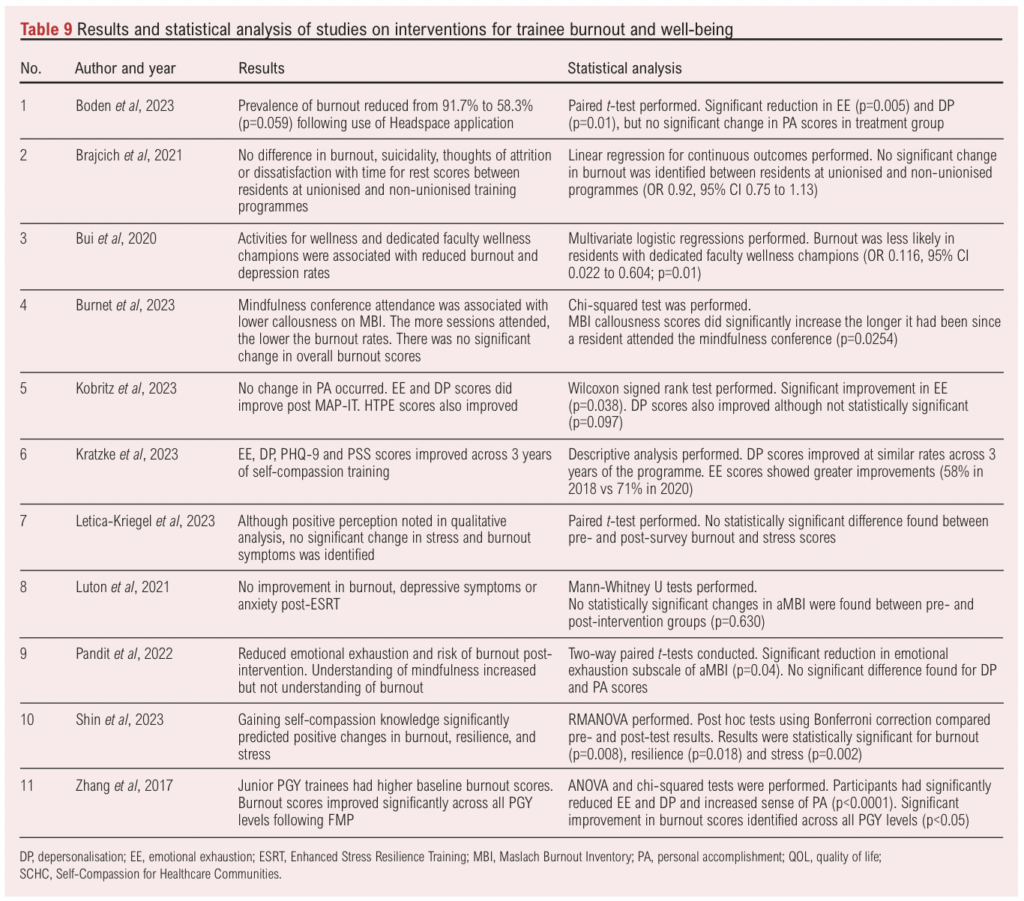
Table 9 summarises the results and statistical analyses from the included studies. No significant changes were observed following intervention in four of the studies.35,39,42,44 All other interventions improved burnout scores in at least one MBI domain.36–38,40,41,43,45
Mindfulness courses
Of the four mindfulness courses, two reduced burnout significantly.36,41 No significant changes in burnout were found in the other two mindfulness studies.39,44
Course delivery varied between a self-directed mindfulness application to mandatory programme-driven initiatives. The ‘Headspace’ mobile app was used for 2 months, and surveys were completed during and following app use completion. The average usage was 8 minutes, 2 days a week. Despite the limited exposure, mindfulness training via the Headspace application resulted in reduced EE and DP scores (p=0.01). In comparison, there was no change in the control group from baseline to 2 months post-treatment.41 The programme-driven initiatives were set up at each institution prior to commencing the studies and comprised various techniques, all following a similar structure. Sessions included dedicated meditation time, group discussion and mindfulness skill-building.36,39,40,44 Sessions in three studies occurred on a weekly basis,40,44,45 one study took place every 6 weeks,39 while the other study did not specify.36 Dedicated faculty wellness champions and wellness opportunities provided by training programmes produced lower burnout rates (p=0.02).36
Mentorship programmes
Both mentorship programmes significantly reduced EE and DP scores.37,43 Mentorship and Assessment of Mentoring and Professionalism in training (MAP-IT) was conducted online via Zoom breakout rooms (Zoom Video Communication Inc. Computer software). MAP-IT mentors met mentees monthly, and the programme consisted of 60 minutes of reflection, reading and open discussion time focusing on humanistic mentoring skills. Following MAP-IT, no significant change in PA scores occurred, although significant improvement was observed in the EE MBI domain (p=0.038). Overall, 46.2% of participants reported a reduction in burnout scores post-MAP-IT (p=0.035).37
The other formal mentorship programme (FMP) did not specify whether the programme occurred online or in-person. FMP encouraged mentors to meet their mentee’s tri-monthly, with supplemental mentors available on an ad-hoc basis. FMP mentors offered guidance on research, surgical, clinical and personal development. Mentorship outcomes were measured at baseline, 3, 6, 9 and 12 months following administration of the FMP. Average baseline MBI scores were initially high (EE: 47.6 and DP: 50.6), with low PA score of 16.5. At 12-month follow-up the scores significantly improved to EE: 14.9 (p<0.0001), DP: 20.1 (p<0.0001) and PA increased significantly to 42.5 (p<0.0001).43
ESRT
ESRT is a secular mindfulness training adapted from mindfulness-based stress reduction (MBSR). The ESRT course conducted in the included study consisted of 1-hour sessions delivered by a qualified ESRT instructor for 5 consecutive weeks.42 Due to the COVID-19 pandemic, ESRT was conducted virtually, which differs from the original ESRT protocol. ESRT reduced overall burnout scores by 38.9%. ANOVA analysis on the effects of ESRT showed potential in reducing burnout rates compared with the control group (mean±SD 5.14±2.35 vs 3.14±2.25; p=0.002).42
SCHC
SCHC is a brief form of the mindful self-compassion (MSC) programme used in healthcare. Both SCHC programmes were led by qualified instructors once a week for 6 weeks and involved several concepts: understanding self-compassion and self-criticism, mindfulness exercises, and tackling stress and burnout.38,45 Both SCHC studies reduced burnout scores post-training.38,45 Descriptive analysis showed no improvement in DP scores after one of the SCHC programmes. However, EE did improve (2018: 58% vs 2020: 71% improvement).38 Similarly, increased self-compassion post-SCHC training significantly predicted burnout reduction (p=0.018).45
Unionisation
One study focused on structural changes in the form of unionisation of surgical training programmes. No significant difference was identified between residents at unionised versus non-unionised programmes.35
Discussion
This scoping review identified 22 studies. Burnout was prevalent regardless of gender, but female trainees may be more at risk due to increased exposure to mistreatment at work. Conflicting evidence was found on the prevalence of burnout across training levels. However, surgical specialty and programme-specific characteristics contribute heavily. Interventions decreasing burnout included mindfulness courses, mentorship programmes, training programme unionisation, and stress, resilience and self-compassion training. Apart from unionisation, all mentioned interventions had some success in reducing burnout.
One mindfulness course elicited no significant difference between pre- and post-survey burnout scores. Perhaps the burnout questions asked were too broad to reflect changes in burnout caused by the process groups.39 Despite showing no significant changes, participants who did not attend any mindfulness conference had higher rates of burnout. This suggests attending even one session may improve well-being and burnout. Lack of significance may be because the mindfulness skills were not exclusively taught to cope with burnout and stress outside of the conference setting.44
Conversely, residents with dedicated faculty wellness champions experienced less burnout (OR 0.116, 95% CI 0.022 to 0.604; p=0.01).36 This study, however, had a low response rate introducing non-response bias. Results may have been overestimated as trainees experiencing burnout symptoms were more likely to respond.
Headspace application use reduced burnout among orthopaedic trainees. This was the only study with a control group enabling a confirmed association to be made. The baseline burnout prevalence (98.5%) in this study was higher than prevalence estimates from previous literature.46 Higher prevalence may be recorded as residents experiencing burnout were more likely to participate. However, findings may be more representative of orthopaedic trainees as survey data were not accessible to the residency programme.41
In comparison, both mentorship programmes reduced burnout. Whilst both FMP and MAP-IT interventions improved burnout and well-being within a short period, the wider training programme environment still contributes to surgical trainee burnout. In the FMP study period, no other major changes were made to the training programme, suggesting the improvements in burnout are attributable to the FMP. Lack of control groups in both studies and participant susceptibility to response and selection bias, due to the cross-sectional study designs, means confounding variables cannot be discounted.
The ESRT study had several limitations. Due to the small sample size, non-response and selection bias remains and, because of the timing of the study, COVID-19 likely influenced the results as the ESRT course was adapted to work around the pandemic restrictions. Generalisability may not be possible due to financial limitations and training programme differences. However, this study was able to reproduce the effects of ESRT previously observed in the USA, implying ESRT is feasible in the UK and potentially across the globe.
Self-compassion training improved self-compassion among surgical trainees and was a predictor of lower burnout but, again, the results may not be generalisable due to small sample sizes and the absence of control groups. As follow-up surveys occurred shortly after post-training, there is a lack of long-term outcome evaluation therefore the results may be exaggerated, although evidence suggests that burnout reduction persists years following self-compassion training.47 In one of the studies, significant improvements in self-compassion were only measured in the self-kindness and mindfulness subscale. Therefore, we cannot confirm improvement in overall self-compassion leads to decreased burnout.45 Despite limitations, the studies increased our insights into how online SCHC programmes reduce burnout and promote well-being in surgical trainees.
Although burnout was not affected, sexual harassment was reported less frequently at unionised programmes. Despite sexual harassment being a predictor of burnout, this correlation did not translate on multivariate analysis. This suggests the reduction in sexual harassment may be attributable to confounding variables not accounted for in this study.35
As this is a new research area, a substantial risk of bias exists with more work required to establish definitive interventions for training programmes. However, the included studies do show promising results. Further research would confirm the effects of these interventions, especially around mindfulness and mentoring at institutional levels. Further controlled trials, specifically involving interventions across multiple sites and incorporating other burnout predictors such as harassment, may help reduce burnout among vulnerable populations.
Limitations
Despite all the included studies using the MBI for burnout assessment, there is no uniform consensus of MBI scoring. Therefore the definition of ‘high-risk’ of burnout varied, as some studies required high scores across all three MBI domains whereas other studies only required high scores in EE and DP domains. This affected the comparability of the studies and introduced heterogeneity in the results of burnout prevalence. Most studies had limited participants and no comparative control group, making it impossible to confirm any identified associations. Non-response and selection bias was rampant across the included studies. Varying locations, differing programme structures and studies involving participants from only one training centre reduced the generalisability of the results.
This review did not consider other important variables associated with burnout such as work hours and environment or personal circumstances. Moreover, the COVID-19 pandemic15,20,24,39,42 would have influenced the number of resources available, work hours and workload – all factors known to contribute to burnout.48–50
Furthermore, the majority of the included studies in this review originated in the USA. Training programmes vary greatly among different countries, especially compared with surgical training programmes in the UK. Surgical trainees in the UK would benefit greatly from introduction of interventions aimed at tackling burnout due to the high prevalence. Balendran et al noted that three out of every five surgical trainees in the UK demonstrated burnout, which is one of the highest reported prevalences.6 Randomised controlled trials should be undertaken in UK surgical training programmes to emphasise the feasibility of these interventions across training programmes in this country.
The association of burnout prevalence with gender was the primary aim in only three studies. Similarly, only one study explored burnout rates among different training levels as a primary outcome. Most studies opted for convenient sampling and did not involve a control group, therefore confounding variables could not be eliminated. Hence, any associations found on burnout prevalence cannot be confirmed. Follow-up times of the implemented interventions were short, with only two studies conducting follow-up surveys at either 1 month post-intervention or 3 months post-intervention completion. All other studies conducted follow-up surveys on intervention completion only. Due to impact bias, the duration of improvement may be overestimated.
Conclusion
Surgical trainees are at risk of burnout, and it is a faculty responsibility to look after their trainee’s well-being during training. This review highlighted that trainees of all genders and training level are unfortunately subject to harassment and increasing prevalence of burnout. Female trainees in particular face greater discrimination, sexual harassment and abuse compared with their male counterparts. More education at institutions on the relationship between negative behaviours and well-being is needed, alongside faculty-led wellness initiatives to reduce burnout. Junior trainees may be at risk of higher burnout due to work hours and poor mentorship, which can be easily remediated through mentorship programmes.
Further research through randomised controlled trials is required to find conclusive associations between both contributing factors on the prevalence of burnout and the effectiveness of the proposed interventions highlighted in this review. A cultural shift towards educating trainees and faculty members on burnout and encouraging peer support can aid the reduction in burnout in surgical trainees.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2024;4(1):5-17
Publication date:
November 22, 2024
Author Affiliations:
1. Warwick Medical School, Gibbet Hill Campus, Coventry, West Midlands, UK
2. University Hospital Coventry & Warwickshire, Clifford Bridge Road, Coventry, UK
Corresponding author:
Aimen Nasim
Warwick Medical School, Gibbet Hill Campus, Coventry, West Midlands CV4 7AL, UK
Email: Aimen.Nasim@ warwick.ac.uk


")

")

