ORIGINAL RESEARCH
Vascular Anastomosis Course for Core Surgical Trainees (VACT)
Condie N,1,2 Al-Saadi N,1,2 Matthews R,1,2 Summerour V,1,2 Wall M1,2
Plain English Summary
Why we undertook the work: Prior to applying for a surgical specialty, surgical trainees complete a two-year programme called core surgical training. Over these two years the trainees are expected to gain understanding of the management of common vascular conditions and have practical experience of vascular surgery. The Vascular Anastomosis Course for Core Surgical Trainees (VACT) aims to provide Core Surgical Trainees (CSTs) with exposure to vascular surgery and the opportunities to develop these skills.
What we did: VACT is a one-day course for CSTs that involves four practical sessions and two lectures. The group size ranges from 10 to 12 for each session. The lectures aim to improve knowledge around common vascular conditions and vascular trauma. This course was held on three separate occasions. An anonymous online survey was distributed before and after the programme. The survey asked trainees about their experience of vascular surgery and to self-assess their confidence levels for each of the different areas.
What we found: Despite undergoing placements on vascular surgery, many trainees do not manage to meet their curriculum objectives. The feedback demonstrated that attending VACT improves knowledge and confidence in practical skills and therefore is beneficial to the trainees and the centres in which they work. Open text feedback was extremely positive, and CSTs reported that they had little exposure to these skills previously and would recommend this course to their colleagues.
What this means: VACT could be replicated in different centres nationally. This would provide CSTs with a better understanding of vascular surgery and encourage them to pursue the specialty as a career..
Abstract
Introduction: On completion of Core Surgical Training, Core Surgical Trainees (CSTs) are expected to have an understanding of emergency and elective vascular conditions as well as practical experience of vascular suturing. A proportion of CSTs will have a vascular rotation and may have been unable to acquire these skills during their placement. We used the postgraduate virtual learning environment (PGVLE) developed by Health Education England West Midlands (HEEWM) in combination with practical sessions to provide a Vascular Anastomosis Course for CSTs (VACT). There are few courses aimed at teaching CSTs the practical skills needed to become a vascular surgeon. VACT aims to improve tissue handling and teach anastomotic technique to CSTs whilst exposing them to the vascular specialty and increasing their knowledge of vascular disease and its management.
Methods: VACT is a one-day course consisting of one hour of online material and a one day in-person session. The online content was distributed via the PGVLE platform and included pre-course video tutorials, information and a survey. The in-person portion of the day included two lectures on vascular surgery and trauma and four practical stations covering embolectomy, inlay grafting, end-to-side anastomosis and patch repair. Course feedback was collected anonymously on PGVLE with automated certificate distribution after completion. The results were analysed qualitatively.
Results: Thirty East and West Midlands trainees attended the course, of whom 25 (83%) completed the post-course feedback. Three had been on a previous vascular course and 15 would consider applying for higher level vascular training. Eight trainees (32%) self-scored their knowledge of common vascular conditions as good/excellent before the course; this increased to 20 (74%) post-course. The number of trainees self-scoring themselves as confident/very confident with vascular emergencies increased from 0 (0%) pre-course to 15 (56%) post-course. The delivery, content and equipment for the practical stations was rated as excellent/good by all participants in the embolectomy station and by 96% of participants in all other stations. Prior to the course one person (4%) rated their practical skills in vascular surgery as good/excellent. After the course this increased to 14 (56%). In all four practical stations, self-rated confidence levels increased after completing the course.100% of attendees would recommend this course to their colleagues.
Conclusion: Feedback from VACT was extremely positive with comments requesting further similar courses. With an increasing need for vascular surgeons, it is essential we provide CSTs with the skills required to complete core surgical training and pursue a career in vascular surgery. VACT could be replicated and adapted to provide vascular training to CSTs across the country.
Background
On completion of Core Surgical Training, Core Surgical Trainees (CSTs) are expected to have an understanding of emergency and elective vascular conditions – specifically acute limb ischaemia, embolic arterial disease and vascular injury.1 These are CST curriculum index conditions that CSTs are required to know how to manage.1 In addition to this, an understanding of vascular suturing and anastomotic technique is expected from the CST curriculum.1 There are a limited number of vascular surgery courses aimed at CSTs in the UK and these can be expensive and have limited availability. Many trainees will not gain any vascular exposure throughout their training due to non-vascular placements. This leads many CSTs to feel that they have inadequate exposure to vascular surgery and therefore do not want to commit to the specialty.2 A survey by Hardy et al has shown that trainees with no previous placements in vascular surgery would not consider applying for the specialty.2 Increasing access to vascular surgery and vascular surgery courses is likely to increase subsequent applications, as has been demonstrated in other specialties.3-6
Since COVID-19, hybrid courses containing online and in-person material have become increasingly popular. The postgraduate virtual learning environment (PGVLE) software developed by Health Education England West Midlands (HEEWM) has been used nationally as a platform for online learning. We aimed to use this in combination with practical sessions to provide a Vascular Anastomosis Course for Core Trainees (VACT). We aim to use case-based discussions and learning from lectures on vascular surgery principles to boost trainees’ knowledge of vascular surgery and its operative techniques. The VACT course aimed to improve tissue handling and teach the anastomotic technique to CSTs whilst exposing them to the vascular specialty and increasing their knowledge of vascular disease and its management.
Methods
The VACT course was designed by West Midlands CST training programme director for training (a vascular surgeon) with experience in developing the vascular course as a course convenor for the Vascular Limb Salvage Academy. The course was designed based on the CST curriculum requirements for vascular surgery knowledge and basic surgical principles of vascular surgery and tissue handling. It involved one hour of online learning to be undertaken prior to the course (demonstration videos and lectures) and a one-day practical session with on the day lectures. We carried out three sessions using the same format over the course of one month. The course was advertised through the PGVLE CST training page and word of mouth.
PGVLE/online portion
Using the PGVLE platform, participants were provided access to pre-course video tutorials covering each of the practical stations, ‘tips and tricks in vascular surgery’ and the extended lecture material. They were asked to complete an anonymous pre-course survey self-assessing their knowledge and practical skills in vascular surgery using the 5-point Likert scale (1: very poor, 5: excellent). The survey also included questions regarding previous exposure to vascular skills courses and potential consideration of a career in vascular surgery. The survey finished with a free text question asking for any specific goals for the course, which was reviewed by faculty prior to the in-person session. Candidates were able to complete the survey at any point before the course date.
Practical session
The face-to-face practical portion of the course was held in a clinical skills laboratory in a vascular hub. Faculty included consultants, vascular surgery registrars and advanced nurse practitioners. Faculty ratio was a minimum of one faculty to two trainees. Each session was made up of 8–12 trainees and at least six members of faculty. The session lasted seven hours. Equipment for the sessions was sourced from clinical skills laboratories within the Black Country Vascular Network, sponsors (Ethicon and LeMaitre) and theatres. A list of all equipment used can be found in Appendix 1 (online at www.jvsgbi.com). The session consisted of two lectures and four practical skills sessions in the format shown in Table 1. Where necessary, one attendee initially started as the assistant and the other as the lead surgeon before swapping over half-way. They were given the opportunity to ask questions throughout the session and carry out the procedure using vascular instruments and encouraged to try equipment (loupes, needle holders, ring tip forceps, etc) with which they often had little or no experience.
A post-course feedback questionnaire was collected anonymously on PGVLE with an automated certificate distributed after completion. We asked candidates to complete this immediately after the course. The survey was linked to the questions asked in the pre-course survey on knowledge and confidence in practical skills in vascular surgery for comparison.
Results
Thirty East and West Midlands trainees attended the course. Of these, 27 completed the pre-course feedback and 25 (83%) completed the post-course feedback.
Prior to the course, three trainees had been on a previous vascular course (12%) and 19 (76%) had undergone a rotation in vascular surgery. When asked in what specialty they would like to pursue a career, 16 said they would consider applying for vascular specialty training.
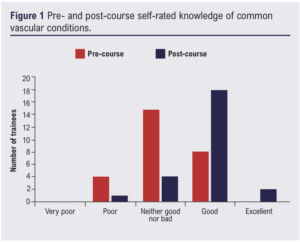
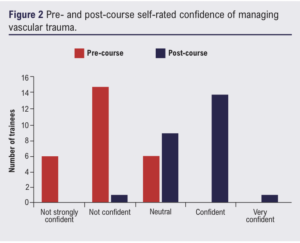
All candidates rated the delivery and content of the lecture ‘Principles of Vascular Surgery’ as excellent/good. Twenty-four (96%) thought the lecture on ‘Bleeding and Trauma in Vascular Surgery’ was excellent/good with one person rating it as average. The lecture content was used to break up the practical sessions and the combination of lectures and practical sessions received positive feedback from the trainees. The delivery, content and equipment for the practical stations was rated as excellent/good by all participants in the embolectomy station and by 96% of participants in all other stations. Figures 1 and 2 show an improvement in confidence and knowledge of common vascular conditions and managing vascular trauma after the course. Eight trainees (32%) self-scored their knowledge of common vascular conditions as good/excellent before the course, which increased to 20 (74%) after the course. The number of trainees self-scoring themselves as confident/very confident with vascular emergencies increased from 0 (0%) before the course to 15 (56%) after the course.
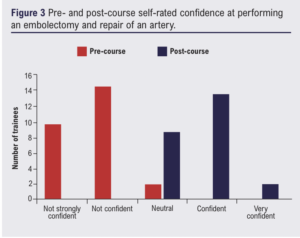
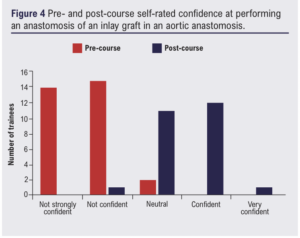
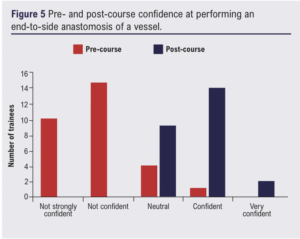
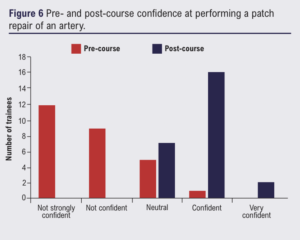
Prior to the course one person (4%) rated their practical skills in vascular surgery as good/excellent, which increased to 14 (56%) after the course. Figures 3–6 show pre- and post-course confidence levels in each of the practical stations. The number of trainees rating their confidence as very confident/confident for each station increased from pre-course to post-course. For embolectomy this went from 0 to 14 (54%) and for aortic inlay graft it went from 0 to 52%. For patch repair of an artery one person (4%) ranked themselves as very confident/confident pre-course, which increased to 18 (72%) post-course. For end-to-side anastomosis, one trainee (4%) ranked themselves as very confident/confident before the course, which increased to 16 (64%) after the course.
Qualitative feedback from candidates
Pre-course material
‘The pre-course videos were great to learn from. The lectures were short, clear and concise’.
‘Theory knowledge online first meant greater focus on practical skills’.
Faculty to trainee ratio
‘The faculty to student ratio was excellent. I was guided by a consultant or registrar for each skill, and I found this extremely useful to receive feedback throughout the course’.
‘Great opportunity to practice and learn with close supervision. Ratio of faculty to student very good!’
The wish for more time
‘Maybe even have it over 2 days and add more practical skills’.
‘Maybe practicing each station twice?’
‘Would have been good to have longer individual time of each specimen’.
Enjoyment of practising practical skills
‘Lots of hands-on practical time which has increased my confidence’.
‘Helped increase my confidence in performing surgical skills’.
‘Run it more often, add more stations’.
‘I feel much more confident in my own skills’.
Overall opinion
‘Probably the best surgical course I have ever been on. I wished we had something like this at the start of CT1. Having considered, faculty feedback on our surgical skills was very valuable. Helped increase my confidence in performing surgical skills. Really enjoyed the lectures, practicals, and food’.
How to improve the course
• ‘Maybe even practising each station twice’.
• ‘Run it more often’.
• ‘Have it over 2 days and add more practical skills’.
• ‘More courses like this’.
When asked, 100% of attendees stated that they would recommend this course to their colleagues.
Discussion
It was felt within the West Midlands Core Surgical Training committee that the opportunities for trainees to access vascular surgery training were limited and that a course would be of benefit. The West Midlands region received its allocation of COVID recovery money and the course was funded through this programme. £6000 was allocated, which allowed for the purchase of equipment to teach, feed and water 30 candidates. Costs will be reduced going forward as jigs required are now purchased and inserts remain relatively cheap. The support from industry also blunted the cost with the use of out-of-date stock and free samples.
The course was over-subscribed, showing a strong desire for a vascular anastomotic and knowledge themed course amongst CSTs. Nineteen trainees who had previously undergone vascular rotations still felt the need to attend the course. This demonstrates that VACT is beneficial to all CSTs regardless of their placements. The course had some secondary aims as well which included giving CSTs the opportunity to talk to vascular surgeons and ask any questions about techniques and opportunities which they may not have had within their core surgical placements. The course therefore also doubled as advertising vascular as a specialty.
Vascular surgery to the non-indoctrinated remains a challenge. The teaching of the basics of vascular assessment can often struggle to get beyond the ‘6 p’s’. The course pre- and post-questionnaires show that the use of multi-media teaching and practical sessions with good availability to knowledgeable faculty can bolster surgical confidence and technique to allow for fulfilment of the vascular part of the core surgical curriculum. 100% of trainees said they would recommend the course. This reflects the need to give trainees access to good training materials and opportunities. With the changes to rotas and ongoing challenges to training that the core group face, this structure of course offers multiple benefits. The course hones knowledge through directed single specialty materials and gives prolonged practical experience which the trainees clearly enjoy and from which they benefit.
VACT could be replicated and adapted to provide vascular training to CSTs across the country. The feedback has shown that it improves confidence in knowledge and practical skills and therefore is beneficial to the trainees and the centres in which they work. Future courses could collect feedback from faculty on the trainees and compare this with the self-assessment scores. They could also look at incorporating virtual reality simulation into the course; this would give trainees objective feedback on the tasks they’re performing. However, setting this up would require initial funding for equipment and training for the faculty.
Courses on teaching basic surgical skills and trauma are already provided nationally and VACT could be rolled out in a similar way. The course administrators did notice the difficulty in getting faculty to volunteer their time for the course, which has been a challenge across the surgical Core Surgical Training since the pandemic and will likely continue to be so.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2024;3(2):71-75
Publication date:
February 9, 2024
Author Affiliations:
1. Department of Vascular Surgery, Black Country Vascular Network, Dudley, UK
2. Vascular Research Innovation Consortium (VaRICS)
Corresponding author:
Natalie Condie
Department of Vascular Surgery, Black Country Vascular Network, Russells Hall Hospital, Pensnett Road, Dudley DY1 2HQ, UK
Email: nataliecondie@ doctors.org.uk


")

")

