CASE REPORT
A deformed Lunderquist wire in a percutaneous endovascular aortic aneurysm repair procedure
Chan DML,1 Gadhvi V,1 Dindyal S1
Abstract
Introduction: An endovascular aortic aneurysm repair (EVAR) is a minimally invasive procedure for repairing an abdominal aneurysm. The advantage of this procedure is that EVAR does not require a laparotomy, hence reducing the physical insult to the body with a quicker recovery time for the patient. Percutaneous EVAR (PEVAR) involves accessing the femoral arteries percutaneously using an access needle without the need of a groin dissection. In this case, a guidewire was damaged and an emergency ‘cut down’ was required to repair the femoral artery.
Case: An 85-year-old woman attended for an elective EVAR. The initial access was gained via percutaneous punctures to both her common femoral arteries under ultrasound guidance. On completion of the procedure the guidewire was removed with difficulty and an emergency right femoral dissection was performed and the common femoral artery was repaired. Postoperatively, the patient recovered well and was discharged the following day after observation.
Discussion: In PEVAR there is no need to make an incision to dissect down to the vessels. Although the vascular closure device comes with an access wire, a standard wire can be passed through; in this case, a stiff wire was used. After removal of the guidewire from the right groin it was found that the wire was severely deformed. It is thought that the wire was caught in the calcium within the vessel.
Conclusion: Although PEVAR is a common procedure, one must be mindful that many factors can affect the endovascular access and closure of the patient. The wire was damaged in this case, either in the femoral artery or in the closure device. It is paramount for vascular surgeons to anticipate that this could be a complication of PEVAR.
Introduction
Endovascular aortic aneurysm repair (EVAR) is a minimally invasive procedure for repairing an abdominal aneurysm. The advantage of this procedure compared with the open technique is that EVAR does not require a laparotomy,1 hence reducing the physical insult to the body with a quicker recovery time for the patient. The conventional EVAR technique generally requires bilateral open femoral artery dissection (‘cut down’). Percutaneous EVAR (PEVAR) is a more recent less invasive approach which involves accessing the femoral arteries percutaneously using an access needle. Like any endovascular procedures, a guidewire is required for the passing of endovascular sheaths and catheters and for the delivery of the stent. A femoral artery closure device is commonly deployed at the end of the procedure to achieve haemostasis, of which there is a wide range available. This report discusses a case in which a guidewire was damaged on removal and an emergency ‘cut down’ was required to repair the femoral artery.
Case report
An 85-year-old woman presented with a 74 mm abdominal aortic aneurysm which was deemed suitable for an EVAR. She had a background of chronic obstructive pulmonary disease with an admission to the critical care unit for non-invasive ventilation in the past. She underwent a preoperative assessment. General anaesthesia was deemed high risk and, following consultation with the patient and her family, the procedure was planned to be undertaken under local anaesthesia and sedation.
Initial access into the abdominal aorta was gained via ultrasound-guided percutaneous punctures to both common femoral arteries. A soft wire was passed via an access needle and Prostar closure devices were passed into each common femoral artery via the guidewires. It was noted that access to the right common femoral artery was difficult at the time due to arterial calcification. Nevertheless, the Prostar closure device was able to pass followed by the sheath and the catheter via the use of guidewires. An aortogram was conducted and the renal arteries were delineated. It was identified that the right renal artery was the lowest. A GORE Excluder device was deployed into the abdominal aorta as the main body of the stent. An iliac contralateral limb was introduced from the left side, preserving iliac blood flow. The left limb was extended, however a completion angiogram showed a possible type 2 endoleak. The main body of the stent was ballooned.
On completion of the procedure the left common femoral artery was closed with the Prostar closure device without problems. However, there were difficulties on removal of the Lunderquist guidewire inserted into the common femoral artery via the Prostar closure device. Once the wire was removed, the puncture site was bleeding. An emergency ‘cut down’ was performed, the common femoral artery was controlled proximally and distally, and the artery was repaired using 5/0 Prolene suture. The subcutaneous tissues and skin were closed with Vicryl and Monocryl sutures, respectively. Postoperatively, the patient was admitted for postoperative care in the critical care unit. She recovered well and was discharged the following day. A 6-week postoperative CT scan showed a decrease in the size of the aneurysm sac from 7.3 cm to 6.9 cm without endoleak and a good position of the stent graft. Her groin wounds healed completely.
Discussion
EVAR has the benefit over open repair in terms of shorter hospital stay, more rapid recovery and early survival.2 As PEVAR does not involve a surgical femoral artery ‘cut down’ it is less traumatic than a standard EVAR. Several studies have shown fewer complications,3 shorter operative time and shorter length of stay,4,5 and these advantages translate into significant reductions in mean hospital costs.6
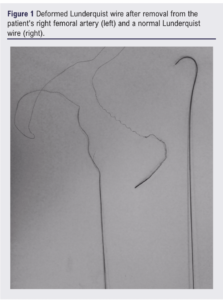
In order to perform a PEVAR, an access needle, guidewire and endovascular closure device are needed in addition to the equipment and devices for a standard EVAR. Although the Prostar device comes with an access wire, a standard wire can be passed through and can be used with the closure device for the procedure. In this particular case a Lunderquist wire was used, which is a stiff stainless steel wire.7 The left femoral artery was closed using the Prostar device without problems. After insertion of a Prostar device into the right femoral artery, it was found that the Prostar device and the Lunderquist wire were caught in the artery. The Lunderquist wire was subsequently removed. On removal it was found that the wire was severely deformed (Figure 1). There was bleeding from the femoral artery and an emergency groin dissection was performed in order to gain haemostasis The wire had been caught in the calcium within the femoral artery.
Conclusion
Although PEVARS are now standard procedures in most vascular units, one has to be mindful of the many factors that can affect endovascular access, closure and haemostasis. In the context of closure after a PEVAR, it is important to keep access to the femoral artery, either with a wire or the closure device, until haemostasis is achieved. Failing this, a surgical repair of the common femoral artery may be required. The Lunderquist wire in this case was caught in either the femoral artery calcification or in the Prostar device. It is paramount for clinicians to recognise that closure devices have a failure rate of approximately 4%,8 and plan for this potential complication of PEVARs, ensuring it is included in the consent process.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2024;3(2):111-113
Publication date:
February 28, 2024
Author Affiliations:
1. Mid & South Essex NHS Foundation Trust, Basildon and Thurrock University Hospital, Nethermayne, Basildon, Essex, UK
Corresponding author:
Deona Mei Lam Chan
Mid & South Essex NHS Foundation Trust, Basildon and Thurrock University Hospital, Nethermayne, Basildon, Essex SS16 5NL, UK
Email: [email protected]


")

")

