WINNING ESSAYS
Rouleaux Club Winning Essay 2025
The Rouleaux Club run an annual essay competition to help promote interest in vascular surgery. Entrants are asked to write 1,500 words on one of three topics selected by the RC Executive. The essays are marked by the committee and the prizes are awarded to the best essay at the annual Vascular Society meeting. There are two prize categories, one for medical students and another for junior doctors. Following the Vascular Societies GB&I Annual Scientific Meeting, the winning essays will be published in the journal.
STUDENT CATEGORY
How can we achieve more timely revascularisation in patients with Chronic Limb Threatening Ischaemia (CLTI)?
Ryan Bloxsom, University of Oxford
Revascularisation is time-critical in Chronic limb-threatening ischaemia (CLTI), with delayed revascularisation associated with excess amputation and mortality.1,2 From symptom onset, there are multiple, sequential delays to revascularisation, with delayed presentation, referral, Vascular review, admission, and revascularisation procedure all contributing to longer time-to-revascularisation (TTR). This essay will explore contributions from each delay to TTR, and identify actionable changes to reduce these delays, and subsequent TTR amongst patients with CLTI.
Facilitating prompt presentation with CLTI symptoms reduces TTR
Delay between symptom onset and primary care (PC) assessment contributes to TTR, being influenced by patient factors, past PC encounters, and appointment availability.3 In a recent interview-based study exploring delays from symptoms to first presentation for CLTI,3 19% of patients identified ‘stoicism’ and 19% identified the perception of the NHS being ‘under pressure’ contributed to their delayed presentation with CLTI symptoms.3 Additionally, past experiences, including frustration with conservative management and lifestyle advice for stable peripheral arterial disease (PAD) contributed to delay in CLTI presentation.3 Patients reported poor awareness of CLTI’s severity, and 25% cited difficulty accessing GP appointments as a cause of delay,3 highlighting patient behaviours, prior experiences, and PC accessibility influence CLTI presentation.3 Safety-netting PAD patients with stable disease, advising immediate re-presentation to PC upon onset of rest-pain, night-pain, ulceration, or tissue loss, may improve patients’ relation with PC, willingness to re-present, and shorten symptom-to-revascularisation time.
Primary care requires further vascular education for timely CLTI recognition
A recent interview-based study with GPs, podiatrists, and practice-nurses explored factors delaying revascularisation amongst CLTI presentations in PC.4 Lack of knowledge of CLTI was evident; 55% self-identified they understood the meaning of CLTI, but 36% of these respondents incorrectly described CLTI when questioned.4 Moreover, 71% of GPs interviewed agreed vascular teaching in PC training is ‘limited’, with 29% believing this impedes timely referral.4 100% of respondents reported referrals were ‘time-consuming’; only 29% felt confident recognising CLTI, and 86% lacked confidence when referring to Vascular for CLTI,4 highlighting a clear need for improved vascular education among PC professionals, promoting early recognition and referral for CLTI patients.
The term ‘chronic’ in CLTI may be unhelpful – 30% of PC professionals interviewed believed CLTI was not an ‘urgent’ condition.4 Whilst underlying atherosclerosis is chronic,5 CLTI onset marks a shift to rapid deterioration and subacute tissue damage.5 Re-branding CLTI as ‘subacute limb-threatening ischaemia’ (‘SALTI’) would be radical, but may better reflect its urgency, distinguish it from stable PAD, and reduce referral delays.
More thorough peripheral vascular examination in PC is needed for timely CLTI identification
Thorough vascular examination, including pedal pulses (PdPs), is critical for timely recognition of CLTI. Despite this, retrospective analysis of PC data from the Clinical Practice Research Datalink identified that amongst 3,260 patients undergoing lower-limb amputation secondary to CLTI, only 7% had PdPs checked in PC in the year preceding amputation, despite a median of 19 PC consultations per patient during that period.6 Moreover, only 2.3% had Doppler ultrasound of PdPs, and 0.2% had ABPI measured,6 suggesting earlier identification of CLTI through vascular examination may prevent amputation. 67% of these patients were seen in PC 7-30 days prior to amputation, although the presenting complaint and discussions during these consultations were not captured.6 For 2025/26, QOF only incentivises PdP-palpation for known diabetics, but not vasculopaths;7 extending QOF-incentives to non-diabetic vasculopaths (e.g. past-MI, stroke/TIA, PAD) may improve early CLTI detection, and reduce TTR.
CLTI referrals should include key signs/symptoms to facilitate appropriate triage to reduce TTR in severe cases
The Vascular Society (VSGBI) outlines an ‘admitted’ pathway for CLTI with rapid progression, deep infection, or uncontrolled pain; and a ‘non-admitted’ pathway for CLTI patients with minor necrosis, controlled pain, or superficial infection, in their quality improvement framework (QIF),8 with indicated target TTR of 5-days and 14-days, respectively.8 In a recent interview-based study, 57% of GPs reported not feeling confident examining for CLTI, 86% did not feel confident referring CLTI, and only 14% suggested examination findings were used to support their decision to refer.4 71% felt Vascular referral forms were helpful, and 29% suggested referral proforma with key referral criteria supported referrals,4 suggesting a standardised referral proforma may guide history and examination, identifying the presence or absence of discriminating symptoms and signs which may influence Vascular triage.
Daily review of referrals in secondary care reduces TTR
Once PC identifies CLTI and refers to Vascular, additional delay is encountered between electronic referral submission (eRS) to triage and outpatient assessment (OPA) by Vascular teams.9 In a recent study of 12 arterial centres,9 eRS review frequency by Vascular teams varied, from daily at 42% of centres, at least every 48-hours in 33%, and weekly in 25% of centres.9 Differences in hubs’ eRS review frequency associated with time to OPA, with centres reviewing daily all achieving OPA within a maximum of 3-days from eRS submission, but those reviewing weekly all experienced a maximum 9-days between eRS submission and OPA,9 suggesting daily eRS review in hubs may reduce TTR by reducing delay to OPA.
Similarly, amongst 10 non-arterial ‘spokes’, daily eRS review was conducted in 20% of centres, with 40% reviewing weekly, and 20% of centres reviewing ‘less-than-weekly’, with only 1 spoke offering emergency, bookable, consultant-led OPAs.9 60% of spokes relied on overbooking emergency OPAs into fully-booked clinics, with one spoke reporting zero emergency OPA capacity.9 70% of spokes offered no ‘hot clinic’, which may contribute to reduced emergency capacity, although these were typically led by Vascular Specialist-Nurses.9 Delays from PC eRS to Vascular OPA could be reduced through more frequent monitoring of eRS submissions, and in spokes offering limited or no emergency capacity, automatic eRS forwarding to hubs reviewing eRS daily may reduce time to OPA and subsequently TTR, but may require patients to travel further for initial OPA and revascularisation. Additionally, if PC have the choice of submitting eRS to a hub or spoke, and both are accessible to the patient, hub referral may reduce TTR through rapid eRS triage, but at the expense of increasing hub caseload and patient travel.
Referral to hubs is associated with shorter TTR than spokes
Delay between Vascular OPA and revascularisation was comparable for hub and spoke OPA, if revascularisation was to take place in a hub, both with a median OPA-to-revascularisation time of 13-days.10 However, since delays from referral-to-OPA, and OPA-to-revascularisation are sequential, total referral-to-revascularisation time is shorter for hub referrals.10 However, if revascularisation was to occur at the spoke, OPA-to-revascularisation time was significantly greater, with a median 26-days, suggesting referral to a hub (if accessible to a patient) may reduce TTR, by reducing referral-to-OPA time, and OPA-to-revascularisation if revascularisation would have occurred in the index spoke, with more than 75% of spoke revascularisations taking longer than the recommended 14-days for revascularisation.8,10 Additionally, a small number of patients presenting for OPA were admitted, discharged, and readmitted – this was associated with a median delay of 33-days,10 reinforcing the idea that discharging CLTI patients from inpatient care should be avoided to reduce TTR amongst this time-critical population.
For patients on the ‘admitted pathway’, hub admissions yield shorter TTR than spokes
Amongst patients on the ‘admitted pathway’ for severe CLTI, Vascular contact-to-revascularisation is significantly shorter in hubs than spokes, with median admission-to-revascularisation times of 5-days and 12-days, respectively.10 Admission to a spoke for inpatient hub-transfer was associated with significantly longer delays (median 12-days), encountering additional 7-days delay versus direct hub-admission, with 81% of patients on this ‘admitted’ pathway failing to meet the inpatient revascularisation within 5-days target, versus 50% for direct hub admissions. This data suggests facilitating patients’ direct hub admission may reduce TTR compared to both spoke-admission for spoke-revascularisation, or spoke-admission for inpatient hub-transfer.10 Patients admitted to either a hub or spoke, who were then discharged for re-admission for revascularisation encountered greater delay of median 20-days from index admission, suggesting patients admitted for CLTI should not be discharged from inpatient care to minimise TTR, preventing an associated 8-days additional delay.10
Additionally, pay-for-performance financial incentives may reduce TTR: a recent single-centre retrospective analysis identified the proportion of CLTI patients revascularised within 5-days via the admission pathway rose from 41% pre-incentive to 59% post-incentive,11 with suggestions that financial incentives engage senior hospital management,11 engendering systematic changes facilitating shorter in-hospital TTR.11 Making these pay-for-performance targets more ambitious over time may encourage continued engagement from senior hospital management, and progressive reductions in TTR.
This essay highlights how TTR in CLTI is influenced by patient presentation, recognition of CLTI, timely referral, urgent Vascular review, and inpatient admission, exploring strategies which could be implemented to reduce each delay and total TTR. During the early stages of CLTI, patient and clinician recognition of CLTI symptoms and urgency of the condition appear rate-limiting factors, with more thorough peripheral vascular assessment in PC essential to increase timely identification of CLTI, to permit prompt revascularisation and reduce major amputation. Delays in secondary care tended to be administrative, with delayed review of referrals and limited OPA availability significantly contributing to overall delay and TTR. Patient and clinician education, thorough vascular assessment plus examination, and streamlined Vascular referral pathways are required to facilitate more timely revascularisation in patients with CLTI.
11. Speirs TP, Atkins E, Chowdhury MM, Hildebrand DR, Boyle JR. Adherence to vascular care guidelines for emergency revascularization of chronic limb-threatening ischemia. J Vasc Surg Cases Innov Tech 2023;9(4):101299. https://doi.org/10.1016/j.jvscit.2023.101299
DOCTOR CATEGORY
How can we achieve more timely revascularisation in patients with Chronic Limb Threatening Ischaemia (CLTI)?
William Jenkins, East of England
Introduction
Chronic limb-threatening ischaemia (CLTI) represents an end-stage manifestation of peripheral arterial disease (PAD)1; characterised by rest pain, non-healing ulcerations (>2 weeks) and/or gangrene.2 CLTI impacts 11% of the 200,000,000 global population with PAD.3 Revascularisation is the mainstay of treatment and is achieved by either open surgery, endovascular intervention or hybrid approaches.4 Prompt identification and revascularisation is paramount as failure to achieve this results in an amputation incidence of ~25%3 and mortality rate of 25-35% at 1-year post-diagnosis.5 The Vascular Society of Great Britain and Ireland’s (VSGBI) Peripheral Arterial Disease Quality Improvement Framework (PADQIF) recommend revascularisation within 5 days for inpatients, and within 14 days for ambulatory outpatients6 due to the significant disease sequelae associated with delayed intervention. Delays to revascularisation occur along the entire referral pathway7 thus there is scope for streamlining the process with targeted interventions to achieve timelier revascularisation.
Demand for vascular services is estimated to increase owing to an ageing population and increased prevalence of diabetes.8 Therefore, this review addresses a prevalent issue with solutions required to improve the significant morbidity and mortality rates associated with CLTI and reduce the ever-increasing burden on healthcare services via achieving timelier revascularisation.
Identifying Community Delays to Revascularisation
To achieve timelier revascularisation, causes of delay along the referral process must be identified and rectified. A systematic review investigating the identification, causes and outcomes of delays in CLTI management attributed delays to both patient and healthcare factors.7
Patient factors included poor health-seeking behaviours and symptom recognition; inevitably resulting in delayed vascular referral.7 This represents lack of lay understanding surrounding PAD and potential sequelae of delayed revascularisation in CLTI. CLTI patient cohorts and those at risk may benefit from targeted educational public health campaigns like the F.A.S.T. initiative for identifying symptoms of stroke and similar initiatives for myocardial infarction. Raising awareness of common signs and symptoms associated with CLTI and the consequences of not seeking medical attention by applying the ‘time is tissue’ mantra to CLTI will likely improve health-seeking behaviours and result in swifter vascular referral.
Primary and community care represents a pivotal initial role in the referral pathway for CLTI. Atkins et al9 sought to evaluate the factors affecting primary care clinicians’ referral behaviours and how these may delay CLTI care. A qualitative semi-structured interview process involving general practioners, community nurses and podiatrists across 12 different vascular surgery units identified several themes delaying CLTI referral. Ambiguity regarding the term CLTI, its status as a distinct entity from acute limb ischaemia and diagnostic thresholds imply CLTI may benefit from a mnemonic akin to 6 P’s for acute limb ischaemia which clinicians expressed more confidence in diagnosing. Another issue voiced was overreliance on ankle-brachial pressure index (ABPI) as an objective proxy of perfusion status and how this can lead to false-reassurance. Apprehension surrounding referring directly to vascular surgeons was also highlighted as a barrier to a streamlined referral process, with negative previous experiences involving ‘sarcasm’ and ‘nervousness about speaking to a specialist’ mentioned. Vascular surgeons must therefore be aware of how they are perceived and the potential repercussions of not being deemed approachable.
An overwhelming theme was how much interviewees felt they would benefit from written guidelines providing clarity on who can refer to vascular specialists. Circulating referral criteria and step-by-step guides on local referral processes to primary and community care staff within regional vascular networks would undoubtedly streamline the process; mitigating any confusion or ambiguity which otherwise may result in revascularisation delay. This was reinforced by participating podiatrists, who generally have greater exposure to CLTI cohorts, expressing more confidence in referring to vascular specialists due to familiarity using tools such as the Wound, Ischaemia, Foot Infection (WIfI) classification10 and European Society of Vascular Surgery calculators to guide referrals more objectively. If this was implemented into common practice when assessing potential CLTI patients in the community it would likely lead to more certainty in referral decisions and swifter contact with vascular specialists. This study also echoed the findings of the systematic review by Nickinson et al7 with patient unwillingness for referral acting as a major barrier to timely revascularisation. Factors contributing to this reluctance need to be identified but is likely due to lack of perceived threat concerning CLTI thus further stressing the need for lay education.
The Hub-and-Spoke Model – Postcode Lottery?
National Health Service (NHS) England has adopted a centralised hub-and-spoke regional model for vascular arterial surgical provision.4 This reconfiguration was introduced following studies which concluded there was a significant relationship between higher-volume hospitals and successful outcomes following arterial surgery.11 Within regional networks, the hub performs arterial surgery and complex endovascular procedures whilst spoke hospitals cater to outpatient services and appropriate day-case procedures.4 Patients requiring arterial surgery who have been admitted to a spoke hospital therefore need to be transferred promptly to the relevant arterial hub.4
A 2022 study found CLTI patients initially presenting to a non-arterial spoke hospital waited more than twice as long for revascularisation compared to those first presenting to an arterial hub4 (Figure 1). This marked discrepancy was however not maintained for those who had initial outpatient assessment at either hub or spoke, followed by admission and revascularisation at the hub hospital.4 This study found that the VSGBI’s PADQIF recommendations of revascularisation within 5 days for non-elective admissions was achieved in 50.3% of patients admitted directly to an arterial hub versus only 18.8% for the spoke transfer cohort.
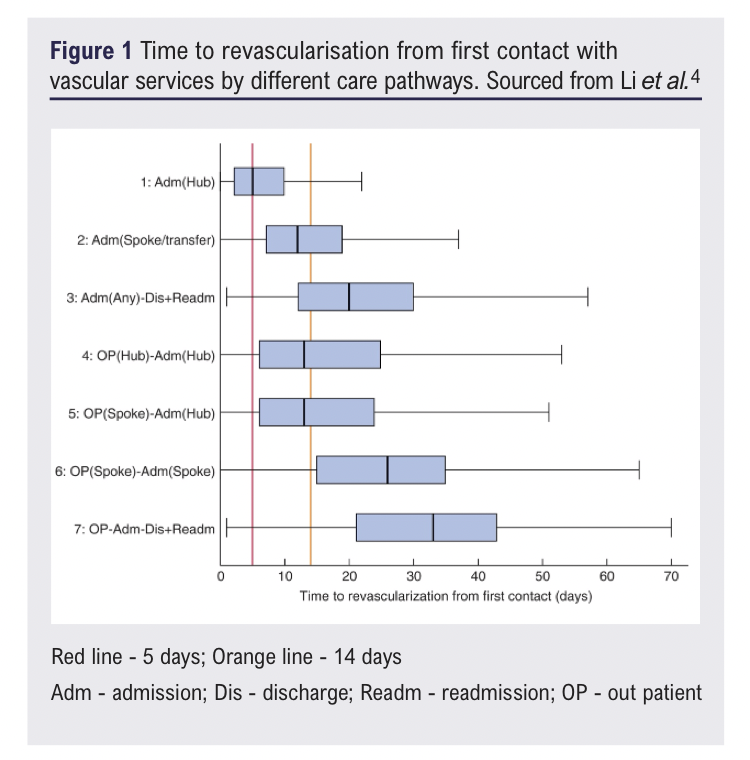
This study identifies an inherent flaw of the hub-and-spoke model in that initial spoke presentation results in unavoidable delay as patients require transfer to the hub for intervention.12 This logistical delay is likely further exacerbated by inpatient hub capacity constraints. Therefore, effective referral pathways within the hub-and-spoke model are paramount to negate the concept of a ‘postcode-lottery’ arising and ensuring timely revascularisation regardless of where a patient presents within a regional vascular network.
‘Hot Clinic’ for Cold Limbs
One concept implemented by some vascular units to try and meet PADQIF recommendations is emergency clinics termed ‘hot’ clinics, whereby CLTI patients receive full clinical assessment including consultant review, laboratory and imaging studies to guide potential intervention6 (Figure 2). Despite hot clinics being recommended in the 2019 Global Vascular Guidelines13 and their use in other specialties being long-established, as of 2021 they were utilised by fewer than 50% of UK vascular units for urgent CLTI assessment.6
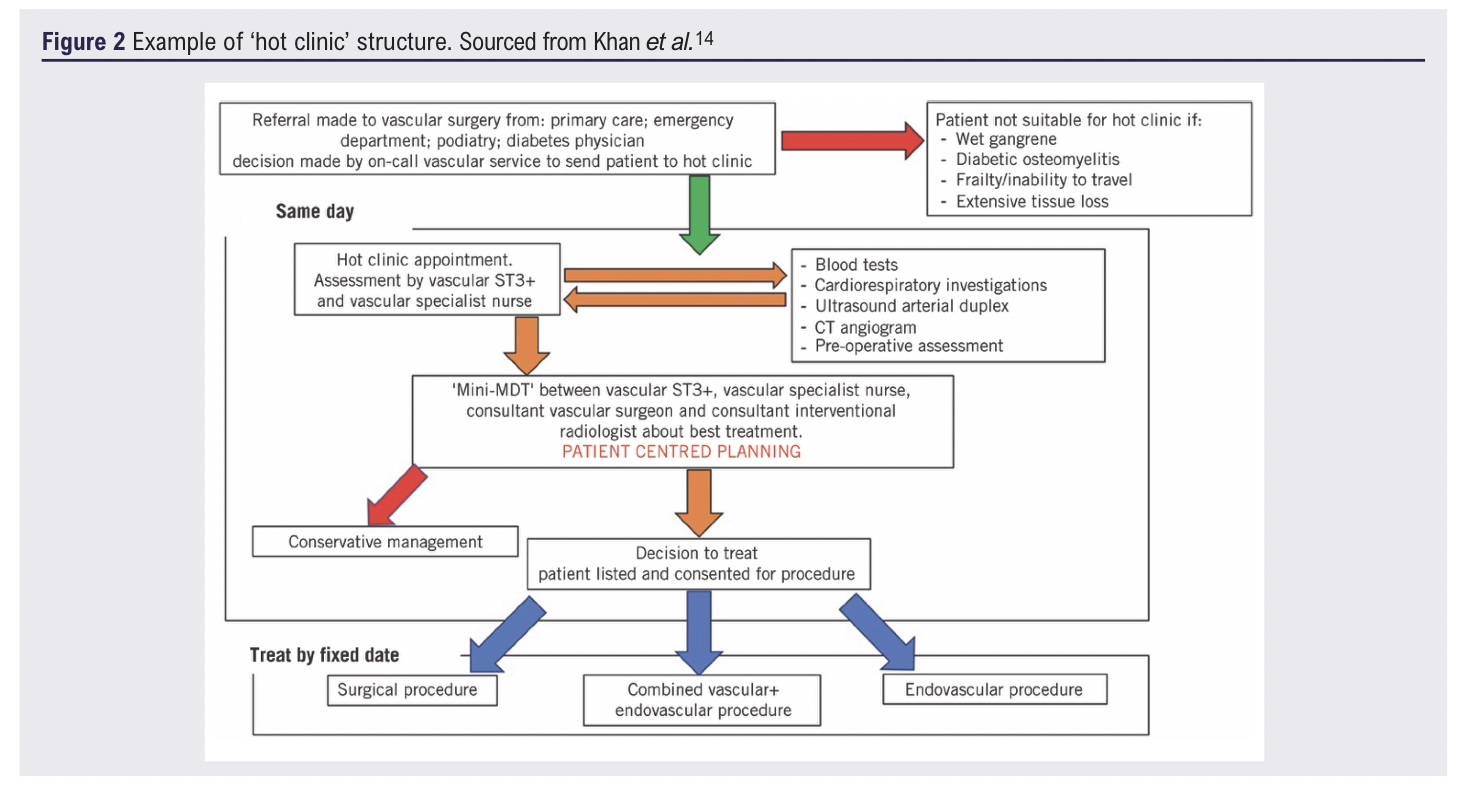
A single-centre prospective cohort study sought to compare outcome measures between cohorts of hot clinic patients versus emergency admissions.14 Whilst there was no significant difference in median time from intention-to-treat to procedure between the cohorts, median time from admission to procedure was significantly lower (0 days) for the hot clinic cohort versus the comparable emergency cohort (3 days). This study also found a significant difference in median length of hospital stay in favour of the hot clinic cohort (3 days versus 17 days) which indirectly facilitates achieving timelier revascularisation for other patients by improving inpatient bed capacity.
The potential role of hot clinics has been given further credence by an observational cohort study with historical controls concluding that 1-year amputation rates decreased from 25% to 11.1% following the establishment of a rapid access limb salvage clinic in a single UK centre.1 Comparison of time to revascularisation between the historical and prospective cohorts could not be directly investigated due to lack of historical data. However, these findings in the context of the implemented rapid access clinic and the established knowledge that timely revascularisation is associated with reduced major amputation incidence suggests hot clinics may well reduce delay in revascularisation and further research is certainly warranted.
The concept of utilising hot clinics to achieve timelier CLTI revascularisation has not been completely adopted nationally and has not yet undergone large-scale investigation but these studies illustrate their potential role. A potential means of further development is establishing small-scale clinics at spoke hospitals (time, personnel and financial provision allowing) with any laboratory and radiological investigations conducted before virtual review, akin to virtual fracture clinics in Trauma and Orthopaedics, by the relevant hub consultant surgeon. This would further streamline the hub-and-spoke referral pathway and reduce the pre-operative assessment and decision-making upon arrival at the hub, resulting in prompt revascularisation and reduced hub burden. Further utilising spoke hospitals as sites for appropriate endovascular intervention and training surgeons to perform more endovascular procedures independently would reduce burden on not only hub hospitals but also interventional radiologists thus maximising existing resources to achieve timelier revascularisation.15 These implementations would somewhat alleviate current issues; ensuring timely revascularisation regardless of where patients present in the hub-and-spoke model.
Conclusion
Delays in CLTI revascularisation are associated with significant morbidity and mortality. Considering disease prevalence is projected to increase, it is critical that methods to achieve timelier revascularisation are identified and implemented. Revascularisation delays occur along the entire referral pathway and thus improvement and education must occur in patient, community and hospital settings. This can be achieved via targeted public health initiatives to improve lay understanding, providing clarity regarding referral criteria for community healthcare professionals, encouraging greater implementation of hot clinics and reallocating certain services to underutilised spoke hospitals.
References
1. Houghton JSM, Meffen A, Gray LJ, et al. Streamlined clinical management pathways may reduce major amputations in patients with chronic limb threatening ischaemia: a prospective cohort study with historical controls. Eur J Vasc Endovasc Surg 2024;69(3):465-73. https://doi.org/10.1016/j.ejvs.2024.09.005
2. Saatzer MD, Jamal AR, Mann ME, Acosta GA, Karagiorgos N. An office-based lab can provide timely interventions for patients with chronic limb-threatening ischemia. JVS-Vascular Insights 2025;3:100187. https://doi.org/10.1016/j.jvsvi.2025.100187
3. Farber A, Menard MT, Conte MS, et al. Surgery or endovascular therapy for chronic limb-threatening ischemia. N Engl J Med 2022;387(25):2305-16 https://doi.org/10.1056/NEJMoa2207899
4. Li Q, Birmpili P, Johal AS, et al. Delays to revascularization for patients with chronic limb-threatening ischaemia. Br J Surg 2022;109(8):717–26. https://doi.org/10.1093/bjs/znac109
5. Holder TA, Gray BH. Clinical decision-making for patients with chronic limb-threatening ischemia. Advances in Surgery 2025;59(1):77-92. https://doi.org/10.1016/j.yasu.2025.04.002
6. A Sivaharan, Brooks M, Bevis P, et al. Models of same-day emergency care for vascular limb salvage. J Vasc Soc GB Irel 2025;4(2):60–3. https://doi.org/10.54522/jvsgbi.2025.163
7. Nickinson ATO, Bridgwood B, Houghton JSM, et al. A systematic review investigating the identification, causes, and outcomes of delays in the management of chronic limb-threatening ischemia and diabetic foot ulceration. J Vasc Surg 2020;71(2):669-681.e2. https://doi.org/10.1016/j.jvs.2019.08.229
8. Kiernan A, Boland F, Harkin D, et al. Vascular surgery workforce: evaluation and estimation of future demand in the United Kingdom. Ann Vasc Surg 2023;89:153–60. https://doi.org/10.1016/j.avsg.2022.08.011
9. Atkins E, Birmpili P, Kellar I, et al. Understanding delays in chronic limb‐threatening ischaemia care: application of the theoretical domains framework to identify factors affecting primary care clinicians’ referral behaviours. J Foot Ankle Res 2024;17(2):e12015. https://doi.org/10.1002/jfa2.12015
10. Mills JL, Conte MS, Armstrong DG, et al. The Society for Vascular Surgery lower extremity threatened limb classification system: risk stratification based on wound, ischemia, and foot Infection (WIfI). J Vasc Surg 2014;59(1):220-34.e2. https://doi.org/10.1016/j.jvs.2013.08.003
11. Awopetu AI, Moxey P, Hinchliffe RJ, Jones KG, Thompson MM, Holt PJE. Systematic review and meta-analysis of the relationship between hospital volume and outcome for lower limb arterial surgery. Br J Surg 2010;97(6): 797–803. https://doi.org/10.1002/bjs.7089
12. Birmpili P, Behrendt C, Boyle JR. Revascularisation for chronic limb threatening ischaemia – the need for speed. Eur J Vasc Endovasc Surg 2023;66(2):158–9. https://doi.org/10.1016/j.ejvs.2023.05.010
13. Conte MS, Bradbury AW, Kolh P, et al. Global vascular guidelines on the
management of chronic limb-threatening ischemia. J Vasc Surg 2019; 69(6):3S-125S.e40. https://doi.org/10.1016/j.jvs.2019.02.016
14. Khan A, Hughes M, Ting M, et al. A ‘hot clinic’ for cold limbs: the benefit of urgent clinics for patients with critical limb ischaemia. Ann R Coll Surg Engl 2020;102(6):412–17. https://doi.org/10.1308/rcsann.2020.0068
15. Nickinson A, Birmpili P, Weale A, et al. What is the current practice for managing patients with chronic limb-threatening ischaemia in vascular surgery services? A survey of UK vascular surgeons. Ann R Coll Surg Engl 2021; 103(9). https://doi.org/10.1308/rcsann.2021.0075
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2025;5(1):49-54
Publication date:
November 26, 2025


")

")

