ORIGINAL RESEARCH
A survey of contemporary acute lower limb ischaemia management
Mannan F,1 Ugwumba L,1 El-Sayed T,1 Saratzis A,2 Nandhra S;1,3 ESTABLISh Research Collaborative and the Vascular and Endovascular Research Network
Plain English Summary
Why we undertook the work: Acute limb ischemia (ALI) is a serious, potentially life- and limb-threatening condition that often results from a sudden blockage in a blood vessel. It requires urgent medical treatment. In recent years, new minimally invasive “keyhole” techniques have been developed, prompting discussion around the best way to treat ALI. This survey was carried out to understand how clinicians currently manage ALI and what treatment approaches they use in practice.
What we did: Between December 2022 and February 2023, clinicians from around the world who treat ALI were invited to complete an online survey. The survey was distributed via email and social media to gather insights into how they diagnose, treat, and manage follow-up care for ALI patients.
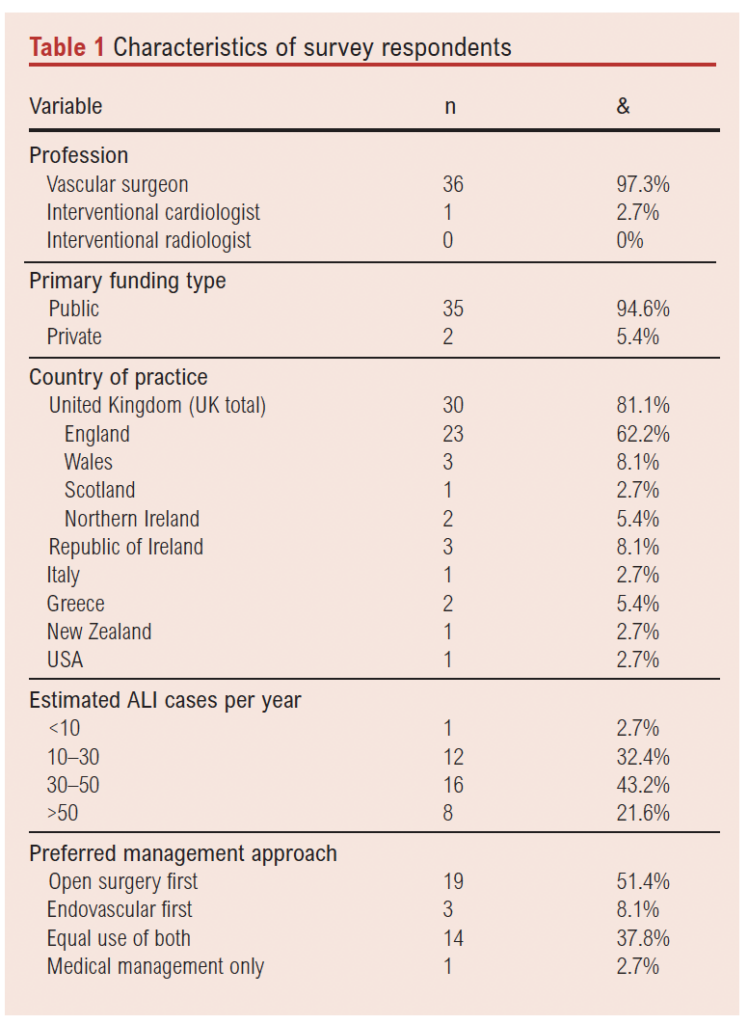
What we found: A total of 37 responses were received from vascular surgeons and interventional cardiologists based in Europe (UK, Italy, Greece), the USA, and New Zealand. Most of the respondents manage more than 30 ALI cases per year. The majority reported using CT scan to confirm the diagnosis and plan treatment.
In terms of treatment preferences:
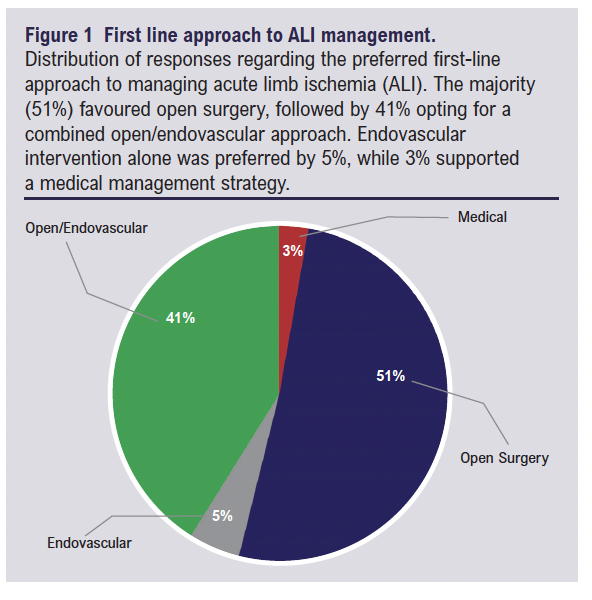
• 51% preferred open surgery, citing confidence in outcomes and concerns over complications such as bleeding and distal embolisation from endovascular methods.
• 5% chose endovascular (keyhole) treatment first, while 40% used both approaches equally, depending on the case.
• 29% supported endovascular techniques as they are less invasive.
• 18% believed endovascular treatment leads to faster recovery.
• 42% reserved endovascular methods for patients with poorer health or limited surgical options.
• 10% made decisions case-by-case, considering factors like the cause of ALI, severity, and expected outcomes.
• For 5%, the availability of specialised facilities (e.g., hybrid operating theatres) and the lead clinician’s preference influenced their choice of treatment.
What this means: There is significant variation in how doctors treat ALI, often based on their experience and available resources rather than strong clinical evidence. Although newer endovascular techniques are gaining interest, many clinicians still rely on traditional surgical approaches. There is strong support among clinicians for further research to determine which treatments work best for which patients.
Abstract
Background: Acute limb ischaemia (ALI) is a limb- and life-threatening condition requiring urgent management. Technological advances have led to the implementation of new endovascular devices into practice. This survey aimed to provide a better understanding of the contemporary management of ALI.
Methods: An international survey was conducted from December 2022 to February 2023 among clinicians who manage patients with ALI using an online survey tool through mailing lists and social media.
Results: 37 responses were received from vascular surgeons and interventional cardiologists from Europe (UK, Italy and Greece), USA and New Zealand. 65% of respondents manage >30 ALI cases annually. Computed tomography (CT) angiography was routinely used for diagnosis and intervention planning.
51% of respondents preferred open surgery for ALI management due to confidence in outcomes and concerns about distal embolisation and bleeding risks associated with endovascular interventions, while 5% preferred endovascular first and 40% used both approaches equally. Approximately 14% of respondents reported lack of endovascular evidence and 5% reported lack of endovascular local expertise.
29% supported the endovascular approach as minimally invasive, while 18% believed it offers faster recovery. 42% reserved the endovascular approach for unfit patients and cases with poor outflow. 10% adopted a selective approach depending on aetiology, clinical severity and predicated endovascular outcome. An interventional radiology room or hybrid availability and leading clinician preference were the key deciding factors for 5% of respondents.
Conclusion: The survey results indicate variation in ALI management, steered by clinician expertise but lacking in level 1 evidence. The appetite for further study was high among respondents and could guide optimal ALI management.
Introduction
Acute limb ischaemia (ALI) occurs as a result of abrupt reduction in limb perfusion due to total or subtotal arterial occlusion by thomboembolism to the peripheral arteries within 14 days of the presentation. It is a vascular emergency with an incidence rate of 140 per million per annum and an average prevalence rate of 1–3%.1,2 ALI severity ranges from a painful limb to complete loss of limb sensory and motor function. This severity range is most commonly classified by the Rutherford Classification.3,4
Although significant advances have been made in the management of ALI, studies to date report high amputation rates of 10–30% at 30 days and mortality rates of 15–20%, hence prompt recognition and emergency treatment is an absolute necessity.5,6 The majority of patients with ALI are aged >75 years and are frail with multiple comorbidities including atrial fibrillation and heart failure, which can influence the management strategy.7,8
Surgical intervention includes urgent lower limb revascularisation procedures such as thrombo-embolectomy and occasionally bypass surgery. These have remained the standard treatments for ALI, but their invasive nature can lead to patient morbidity such as wound infection.9 Patients in whom the limb is deemed unsalvageable as a result of severe ALI are offered a major amputation and/or palliation.10,11
Minimally invasive procedures include percutaneous catheter-directed thrombolysis, which have previously been studied, and modern endovascular thrombectomy techniques with a less definitive evidence base. Modern endovascular techniques aim to reduce the thrombotic burden by thrombus fragmentation, aspiration or rheolytic thrombectomy via a percutaneous approach.12
Historical data exist for catheter-directed thrombolysis, but reliance on this technique is still uncertain within contemporary practice for ALI.13,14 Modern endovascular techniques are being increasingly adopted within the vascular armamentarium, with promising safety data.15-20 However, these data are limited to registries, observational studies or small trials without comparison with surgery.
The suggested advantages of the modern percutaneous interventions are faster restoration of circulation, diagnostic imaging to guide onward management, reduced adverse events of thrombolytic medications (bleeding) and avoidance of risks of open surgical procedures and general anaesthesia.12 These benefits, coupled with increasing availability, have potentially increased the treatment options for patients with ALI, especially in those with comorbidities or frailty that might prohibit gold standard open surgery.
This global survey seeks to explore the current practices in the management of ALI, focusing on the endovascular modern techniques as well as the rationale and follow-up protocol in this modern endovascular era.
Methods
Study design
An international survey was conducted from December 2022 to February 2023. Clinicians who manage patients with ALI were invited to complete an online survey through mailing lists and social media. This survey is reported with reference to the Checklist for Reporting of Survey Studies CROSS.21
Survey design
The survey was developed and reviewed by the lead authorship group. This was finalised and then peer-reviewed by the Vascular and Endovascular Research Network (VERN) before dissemination.
Survey respondents
The survey was aimed at clinicians managing ALI globally including vascular surgeons, interventional radiologists and cardiologists. Participating healthcare professionals were invited to share their contact details and institution for any future research.
Survey objective
The main objective of the survey was to determine how clinicians manage patients with ALI. This included the treatment preferences (such as open versus endovascular interventions) and the reasoning behind selecting one method over another. The secondary outcomes were the type of imaging used before and after interventions, the follow-up (including surveillance) and anticoagulant/antithrombotic regimens. The survey also evaluated ALI research participation and equipoise.
Survey tool
Data were gathered using the JCIS online survey tool (Bristol, UK). The survey captured the respondent’s healthcare setting and location. Respondents were asked to confirm that their response reflected the approach of the unit/centre/institution. The survey evaluated the treatment of ALI, postoperative protocols and their willingness to participate in future studies related to endovascular ALI intervention. The survey questions are shown in Appendix 1 online at www.jvsgbi.com.
Distribution
The survey was distributed through social media platforms and mailing lists via Twitter (X) and newsletters in conjunction with VERN, and responses were collected between 20 December 2022 and 20 February 2023. Only responses within this timeframe were considered in the data analysis.
Data analysis
Data submitted by duplicate responders from the same centre were checked for similarity before being included in the analysis and discrepancies were addressed by contacting the respondent directly. Responses were representative of the approach of a single centre/institution to ALI management. Descriptive statistics, including counts and frequencies, are reported where appropriate. Free-text responses of clinicians’ opinions were collated and described.
Results
Respondent demographics and volume
A total of 37 responses were received from 30 vascular centres globally across Europe, USA and New Zealand. Nearly 95% of these institutions are publicly funded. Only one respondent was an interventional cardiologist (but still represented their unit level practice) while the remaining 36 were vascular surgeons.
Eight of the 37 respondents (21.6%) managed more than 50 cases annually, while 16 (43.2%) managed 30–50 cases and 12 (32.4%) estimated that they reviewed about 10–30 patients with ALI. Only one participant estimated that their unit managed less than 10 cases of ALI per year (Table 1). All the centres used CT angiography as their cross-sectional imaging of choice for assessing ALI.
Responses regarding the approach to management of ALI
Although a correlation between case volume and treatment modality preference was explored, no significant trend was observed due to the limited sample size. Regarding the intervention of choice, 19 of the 37 participants (51.4%) would adopt open surgery while 15 (40.5%) would approach using open or endovascular surgery equally. Only three participants (5.4%) would use the endovascular approach as first choice while one (2.7%) would manage medically with anticoagulants alone (Figure 1).
Reasons for preferred intervention of choice
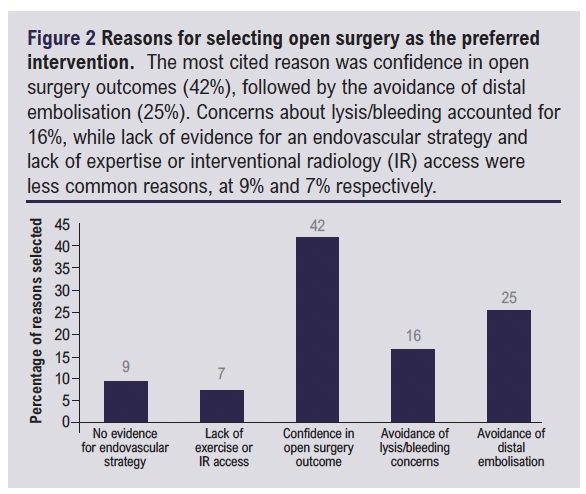
Open surgery
When we explored why respondents would consider an open strategy as the first choice of intervention, the majority (42%) cited ‘confidence’ in open surgery and in its outcome (Figure 2). Meanwhile, fear of distal embolisation (25%) and bleeding risks (16%) were the major concerns for adopting endovascular approach first.
Endovascular intervention
We also explored the reasons why the endovascular strategy is considered the first choice of management of ALI for some (Figure 3). Roughly one-third (31%) of the rationale was because it is less invasive and about one-quarter (23%) suggested that a relatively faster recovery was observed. Patients with poor fitness for open surgery (23%) and those with poor outflow (20%) were the other major reasons for employing endovascular intervention.

Use of on-table completion angiogram following open surgery
When respondents were asked if in their unit they would perform an on-table completion angiogram following an open surgery, five (14.7%) would always perform this but 17 (50%) would only do this when there is no clinical intraoperative improvement of the ischaemic limb or concerns about suboptimal revascularisation. The remaining 12 respondents (approximately 35%) would not perform on-table angiogram investigation, 10 (29.4%) due to logistic reasons and two (5.9%) do not think it is necessary.
Use of anticoagulants and antiplatelets post intervention
Open surgery
All participants would consider at least an anticoagulant or antiplatelet for post-surgical management of ALI. Twelve specialists (35.3%) would usually prescribe only anticoagulant medication, nine (26.5%) would routinely offer a combination of an antiplatelet and treatment dose anticoagulant medication while four (11.8%) would prescribe a combination of an antiplatelet and a prophylactic anticoagulant treatment. The regimen used by the remaining nine respondents (26.5%) would depend on the aetiology.
Endovascular intervention
Similarly, all participants would consider at least an anticoagulant/antiplatelet for post endovascular management of ALI. Seven respondents (41.2%) would routinely medically manage with only anticoagulants, three (18.8%) would routinely offer a combination of an antiplatelet and a treatment dose anticoagulant while two (12.5%) would offer a combination of an antiplatelet but with prophylactic anticoagulant treatment. However, four specialists would adapt their regimen depending on the case/aetiology.
Follow-up investigations and surveillance
Open surgery
Following open surgery for ALI, 14 respondents (41%) do not routinely offer follow-up investigations while eight (23.5%) would usually arrange for a one-off ultrasound arterial duplex. Four respondents (11.8%) would monitor their patient through an ultrasound arterial duplex surveillance programme and only one (2.9%) would perform cross-sectional imaging. The remaining seven respondents (18.9%) would offer follow-up imaging on a case-by-case basis depending on the type of revascularisation (stent/bypass), clinical status and ankle-brachial pressure index.
Endovascular intervention
We also asked all the 16 respondents in the endovascular group if they would offer follow-up imaging. Eight (47%) do not offer routine follow-up imaging and five (29%) would routinely perform a post-intervention ultrasound arterial duplex, of which three often perform this as a one-off investigation while two would place patients on the surveillance programme. The remaining three respondents would approach this on a case basis depending on clinical outcome/patient-specific concerns.
Availability of hybrid theatres
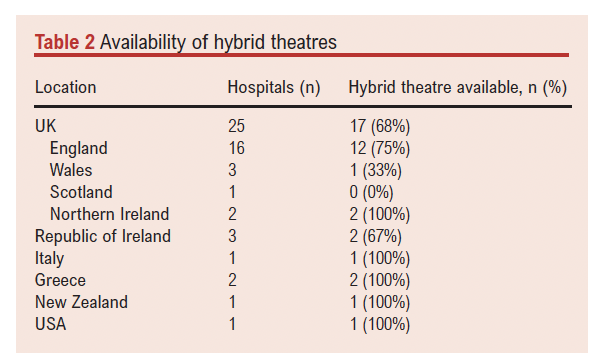
Of the 30 hospitals represented in the survey, 22 (73%) had hybrid theatres. Table 2 further shows the availability of hybrid theatres based on the individual hospitals and regions represented in the survey. Only one hybrid theatre in Wales was not available during out of hours.
Further research and equipoise
We enquired about potential barriers in recruiting patients for future studies in each respective centre and three foresaw no major barriers. However, the lack of research time/staff/resources was the main barrier foreseen by 15 participants (40.5%) and lack of expertise for endo-interventions was a concern for 11 centres (29.7%). Nine (24.3%) expected that lack of equipoise would be an issue while the remaining two predicted a challenge of randomising these emergency cases during out of hours. The majority of participants (89%) were keen to partake in a randomised study of an endovascular versus open first strategy for revascularisation in patients with ALI.
Discussion
This survey shed some light on the contemporary management of ALI across a variety of countries. While severity stratification using the Rutherford Classification could have enhanced the analysis, this was not captured in the survey tool and remains an area for future research.
The breadth of the survey offered a panoramic view of international practice, but this may have limited the depth of data in specific domains such as antithrombotic strategy or follow-up imaging. Several imaging methods can determine occlusion sites in limb ischemia, such as ultrasound, CT angiography, digital subtraction angiography, conventional angiography and magnetic resonance angiography.9 Notably, our survey found that CT angiography emerged as the preferred diagnostic imaging technique. This aligns with numerous studies demonstrating its high sensitivity and specificity for identifying arterial occlusions, providing precise anatomical site information, and its suitability for emergency settings due to its widespread availability in most centres.22,23 This is also in line with the European Society for Vascular Surgery (ESVS) guideline for ALI, which recommends CT angiography as the first-line modality for anatomical imaging.9
Half of the specialists engaged in ALI treatment tend to favour open surgical revascularisation as a first choice owing to their established competency and concerns regarding complications of endovascular techniques, while others were willing to adapt new endovascular techniques equivalently or selectively. The current ESVS guideline recommends surgical thrombo-embolectomy as the standard treatment of ALI caused by embolic occlusions in an otherwise normal artery.9 However, it appreciates that this cohort of patients is becoming increasingly rare as most surgical patients will also have concurrent vascular disease. Regarding evidence for modern endovascular procedures, there is lack of powered clinical trials demonstrating the efficacy and cost effectiveness compared with current surgical practice.9 In addition, the available comparative randomised clinical trials were published in the 1990s, which does not reflect current practice.13,24 Hence, the paucity of level 1 comparable evidence and current recommendations to consider either approach9 could explain the clear division between the intervention techniques noted in the survey.
On-table completion angiography was not routinely performed by most surgeons following open surgical intervention except when there is a suspicion of inadequate or poor distal vascularity. This procedure is typically conducted to confirm full clearance of the arterial tree and distal patency, thus verifying the success of the performed procedure.25 Research indicates that employing routine intraoperative completion angiograms, as opposed to selective use, has a positive impact on revascularisation outcomes, resulting in lower rates of re-occlusion.26,27 In addition, the current ESVS guideline for ALI recommends a completion angiogram irrespective of the intervention method.9 Also, following open surgery, about a third of surgeons do not offer a completion angiogram and nearly two-thirds of these surgeons do not have access to hybrid theatres. This is concerning as the availability of a hybrid theatre is essential for centres to be able to offer this emergency service, and our survey provides information to regulatory bodies to enhance patient care.9,28
Most of the respondents believed in prescribing antithrombotic agents as single or combined therapy. The VOYAGER PAD trial demonstrated that low-dose rivaroxaban with aspirin reduced the incidence of adverse major limb and cardiovascular events. Although bleeding risk was increased in patients with this regimen, this was without significant fatal bleeding.29 A small group of patients with ALI in the COMPASS trial demonstrated similar benefit.30 However, ALI was not the primary focus in these recent trials and there is a need for a focused randomised clinical trial on the management of ALI.9 Our current practice has largely been derived from extrapolating findings from cardiology results and broad groups of patients with peripheral arterial disease.9,31,32
ESVS guidelines specifically recommend long-term anticoagulant cover following ALI revascularisation secondary to an embolus. On the other hand, ESVS recommended the use of either long-term antiplatelet or anticoagulation to reduce cardiovascular events following ALI revascularisation secondary to native artery thrombosis/popliteal aneurysm/failure of previous revascularisation.9 These recommendations and lack of level 1 evidence for patients with ALI could explain the heterogeneity seen in current clinical practice.
CLARITY is an ongoing NIHR funded randomised controlled trial looking at the clinical efficiency and cost effectiveness of three different antithrombotic regimens following peripheral arterial endovascular revascularisation.33 However, this is focused on patients with chronic limb threatening ischaemia (CLTI) which is a different subgroup of peripheral arterial disease with different aetiology, pathology and management principles. There is a need for a systematic review and potentially similar high-powered randomised clinical trials on clinical outcome of the new current endovascular management of ALI to guide current practice.
Post-intervention follow-up varied in our survey, with nearly half of the respondents not routinely offering follow-up investigations while nearly a quarter would perform this routinely. Only a few would initiate a surveillance programme after the intervention. It is not surprising that ultrasound arterial duplex seemed to be the investigation of choice as it is non-invasive and the recommended imaging modality of choice in our current clinical guideline.9 However, the ESVS guideline appreciates that imaging is required if there are clinical concerns during follow-up, but recommends routine imaging follow-up only for patients treated for popliteal artery aneurysm.9 A recent meta-analysis did not demonstrate any difference in clinical outcome when ultrasound arterial duplex was compared with clinical assessment following infrainguinal vein bypass.34 The lack of a definitive protocol observed in the survey is a reflection of current evidence and clinical guideline suggestions.
Nearly three-quarters of respondents had access to hybrid theatres, indicating an increasing availability of a hybrid set-up with 24-hour access. However, in the UK, less than two-thirds of hospitals in the survey had access to a hybrid theatre despite being an established clinical standard for providing this emergency service,28 but some centres that do not have a hybrid theatre may also have access to an interventional radiology suite. Also, the lack of interventional radiologists in our survey might have underrepresented access to the interventional radiology suite. Patients need to have access to both open and endovascular interventions in a single procedure to have a potentially better clinical outcome.9,26
This survey has been insightful, but the relatively small number of centres without representation from interventional radiology does add caution to the overall generalisability of interpretation.
Study limitations
This study has a few limitations including the small number of heterogeneous respondents and vascular centres represented. Additionally, the relatively small sample size, lack of responses from interventional radiologists and the absence of Rutherford Classification data limit the granularity and generalisability of findings.
The online survey methodology carries a risk of sampling and response bias with limited accessibility to the questionnaire. There is always a risk of limiting the depth of responses and the ability to gather contextual details despite our best offer to mitigate this in survey questions.
The future
Rather than providing greater clarity on current practices, this survey has perhaps raised more questions and highlighted diverse clinical practice and paucity of evidence to guide clinical practice. There have been numerous research studies on chronic limb-threatening ischaemia and peripheral arterial disease, but there is minimal research on the subgroup of ALI which has a different aetiology and pathology. The ESVS guideline on ALI recognises that the clinical efficiency of these modern endovascular techniques remains an unresolved issue, and there is a suggestion for patients receiving these modern interventions to be enrolled in clinical trials.9
Completion on-table angiography should be practised in all centres offering management of ALI, as supported by current evidence and ESVS guideline recommendations. There is a need for further studies to guide post-intervention anticoagulant regimens and vascular imaging.
Conclusion
This study sheds a contemporary light on the perspectives of the centres managing ALI. It highlights the growing acceptance of endovascular techniques for ALI treatment, either independently or in hybrid approaches, reflecting a desire for more facilities supporting these methods. ALI is well known to have a significant mortality risk and complications, hence future research comparing open and endovascular techniques in the treatment of ALI is vital.

Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2025;4(3):144-150
Publication date:
May 29, 2025
Author Affiliations:
1. The Northern Vascular Centre, Freeman Hospital, Newcastle, UK
2. Leicester Vascular Institute, Leicester, UK
3. Population Health Sciences Institute, Newcastle University, Newcastle, UK
Corresponding author:
Tamer El-Sayed, NIHR Clinical Lecturer in Vascular Surgery, The Northern Vascular Centre, Fourth Floor, Freeman Hospital, Freeman Road, High Heaton, Newcastle upon Tyne NE7 7DN, UK
Email: [email protected]


")

")

