CASE REPORT
Aberrant retro-psoas course of the left common iliac artery on CT
Tufts M,1 Pietroski A,2 Al-Katib S2
Abstract
Retro-psoas course of the common iliac artery is an extremely rare anatomical variant with important procedural implications. In this case report we describe a 60-year-old man who presented with acute abdominal pain and was found to have a left common iliac artery traveling posterior to the psoas major muscle. Imaging also revealed a high aortic bifurcation at L3 and associated ipsilateral anomalies including a tortuous external iliac artery, absent or poorly visualised internal iliac artery, and the ureter travelling with the iliac vein rather than the anomalous artery. Recognition of rare vascular anomalies like this retro-psoas course is critical for radiologists and surgeons to ensure safe surgical and endovascular planning. Additional vascular mapping is recommended prior to any pelvic procedures in such cases.
Introduction
The common iliac arteries follow a predictable and well-described anatomic course. The abdominal aorta bifurcates into left and right common iliac arteries at approximately the L4–L5 vertebral level. Each common iliac artery travels inferiorly along the anteromedial surface of the psoas major muscle before dividing into the external and internal iliac arteries at the level of the sacroiliac joint.1 This anatomic relationship with the psoas muscle, ureter and adjacent neurovascular structures is typically consistent.
Deviations from this course are exceptionally rare but may have important clinical and procedural implications. Unrecognised anomalies may increase the risk of complications during abdominal or pelvic surgery, as well as during endovascular interventions.2,3 It is important to recognise these variants on imaging to avoid unexpected problems during procedures.
A retro-psoas course of the common iliac artery is among the rarest of vascular anomalies. In this variant the artery passes posterior to the psoas major muscle rather than along its anteromedial surface. A systematic review identified only nine previously reported cases.4-12 We present this case to add to the limited literature on this variant and to highlight the imaging features that allow prospective identification, which has direct implications for surgical and endovascular planning.
Case report
A 60-year-old male with past medical history of chronic pancreatitis presented to the emergency department with a six-hour history of epigastric abdominal pain radiating to the back, associated with chest pain, nausea, and multiple episodes of non-bloody, non-bilious emesis. He endorsed regular alcohol use. The patient underwent a CT of the abdomen and pelvis which demonstrated sequela of chronic pancreatitis with mild peripancreatic fat stranding, suggestive of superimposed acute interstitial pancreatitis. A 2 cm pancreatic pseudocyst was identified.
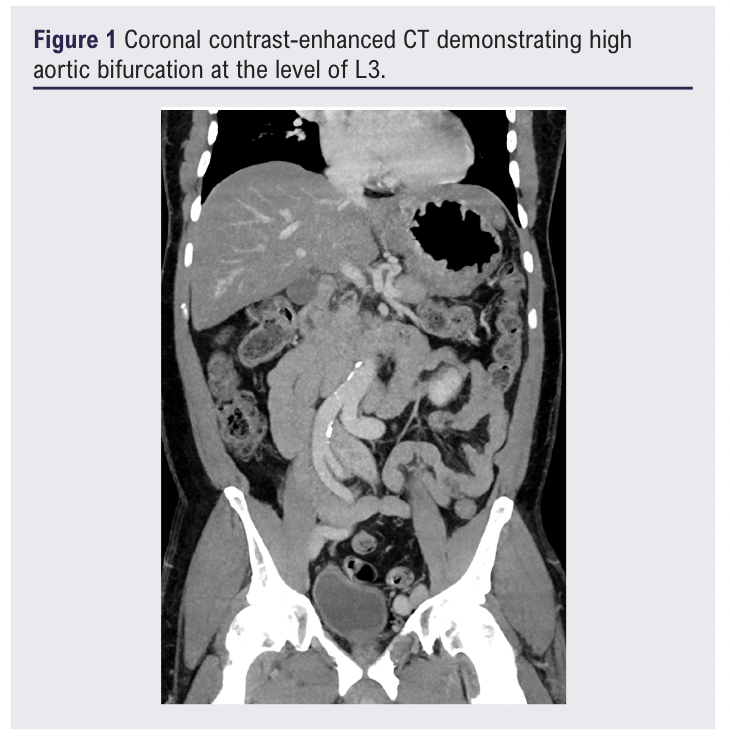
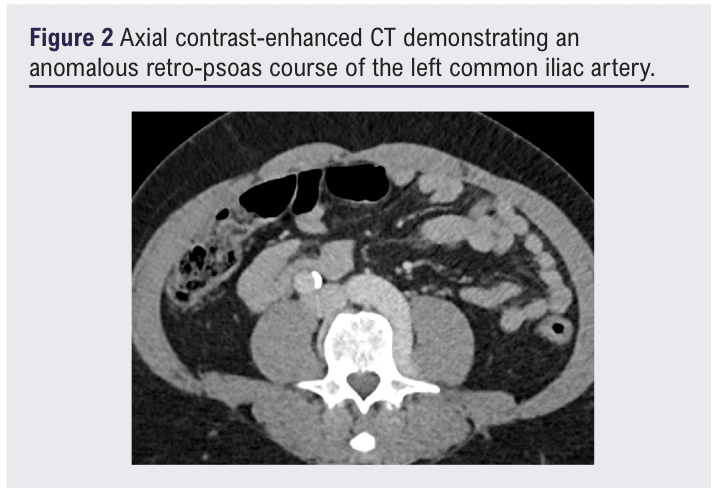
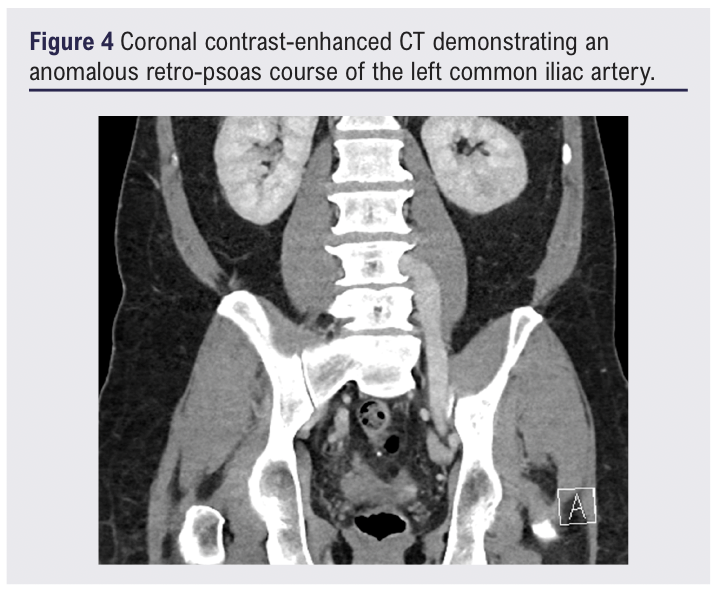
In this patient the aortic bifurcation occurred at the level of L3, superior to the expected L4–L5 level (Figure 1). The left common iliac artery followed an anomalous retro-psoas course, passing against the anterior lumbar spine and sacrum over approximately 8 cm, markedly more posterior than the right iliac system (Figures 2–4), which bifurcated normally at its expected level.
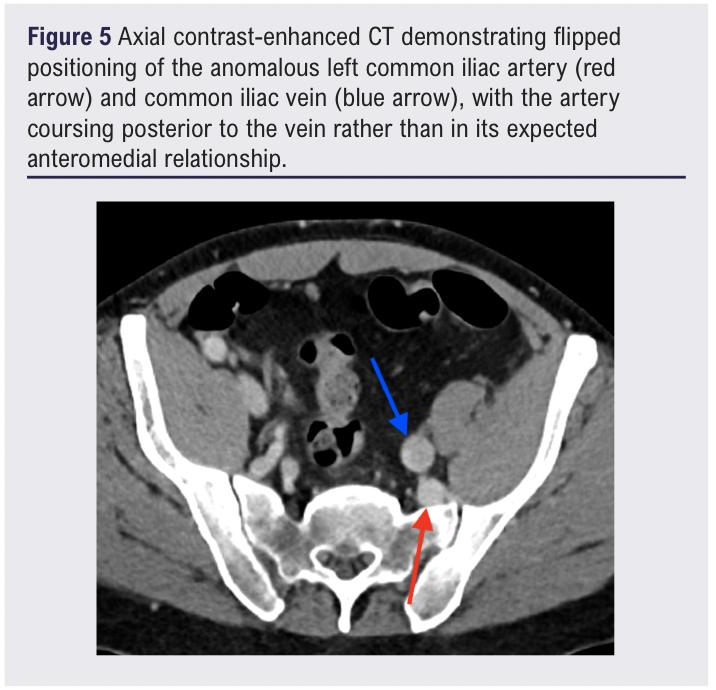
The left common iliac bifurcation was not clearly identified. Small posteriorly projecting branches were present, presumed to represent anomalous internal iliac branches (Figure 5). The left external iliac artery was tortuous, coursing posterior to the left common iliac vein before resuming a more anterior normal configuration distally (Figure 5).
The left common iliac artery demonstrated short segment fusiform dilation measuring up to 1.6 cm in maximum diameter. For comparison, the right common iliac artery measured 1.2 cm, within normal limits. The external iliac arteries were within normal limits of maximum diameter.
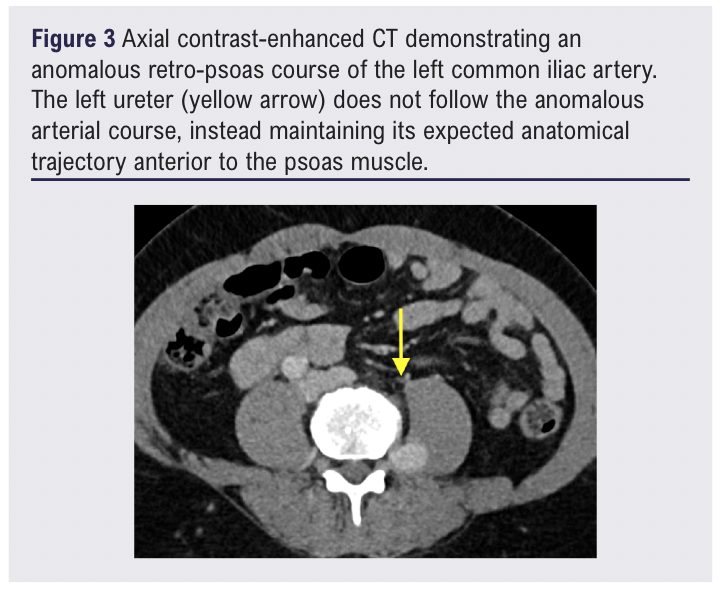
No asymmetric atherosclerosis, stenosis, occlusion, dissection or extrinsic compression was identified. The left ureter followed a normal course alongside the psoas muscle and iliac veins, passing under the vas deferens and inserting normally without hydronephrosis (Figure 3). The right iliac system was normal.
Discussion
Anomalies of the iliac vasculature are exceedingly rare. A retro-psoas course of the common iliac artery was first described in 1991, with only eight additional cases reported since. All documented instances describe a unilateral anomaly with normal contralateral iliac anatomy, and both left-sided and right-sided variants have been reported.4-12
In early embryonic development, paired dorsal aortas run alongside the neural tube before fusing in the midline to form the descending aorta. Their lowermost portions remain unfused, and it is from these caudal segments that the iliac arteries arise. The level at which fusion terminates determines the position of the aortic bifurcation.13,14 An early bifurcation at L3 is therefore a developmental variant. Notably, four prior cases share an aortic bifurcation at the L3–L4 level, suggesting this may be a recurring associated finding rather than coincidence and raising the possibility of a shared embryologic mechanism.4,6,7,11
Between the fourth and sixth weeks of gestation, the common iliac, internal iliac and external iliac arteries are forming simultaneously from the same embryologic source. During this period the dorsal aortas are fusing, the umbilical circulation is being established and the primitive iliac branches are acquiring their definitive positions within the developing pelvis.15 A single developmental disturbance during this window most likely explains the full spectrum of left-sided anomalies seen in this case.16
The precise mechanism by which the common iliac artery comes to lie posterior to the psoas muscle is not fully understood, but several explanations have been proposed. The common iliac artery and the psoas muscle form at the same time and in close proximity to one another. As they grow, the artery normally settles into a position in front of and to the side of the psoas.17 One explanation is that the artery establishes its course too early, before the psoas has finished moving into its final position. The psoas descends and rotates forward as it matures, and if the artery is already fixed in place when this happens, the muscle could effectively sweep in front of the artery, leaving it stranded behind. Another possibility is that the artery itself simply grows in the wrong direction from the start, tracking posteriorly rather than anterolaterally, possibly due to abnormal signaling in the surrounding tissue.
This case also illustrates an important principle regarding ureteral landmarks in the setting of anomalous pelvic vasculature. The ureter classically crosses anterior to the common iliac artery at the pelvic brim, a relationship routinely relied upon in urological, gynaecological and colorectal surgery.18 In this case, the left ureter follows the course of the iliac vein rather than the artery. Ureteral position cannot be inferred from arterial landmarks alone when iliac anatomy is anomalous, and dedicated assessment of the ureteral course on preoperative cross-sectional imaging is warranted in all such cases.19
In this case, the retro-psoas left common iliac artery is accompanied by several ipsilateral anomalies. No clearly defined left internal iliac artery is identified. The left external iliac artery is tortuous with an inverted positional relationship to the common iliac vein, and multiple small posteriorly projecting arterial branches are present whose course remains uncertain. Three possibilities are proposed for the pelvic visceral blood supply: direct branches from the common iliac trunk; a hypoplastic internal iliac artery with anomalous branching; or an accessory internal iliac configuration. This distinction has direct clinical consequences as prostatic and uterine artery embolisation, internal iliac occlusion during endovascular aortic repair and pelvic surgical ligation all require reliable internal iliac mapping before proceeding.3 Conventional angiography or dedicated thin-slice CTA with multiplanar pelvic reformations would be beneficial prior to any pelvic intervention.19
Conclusions
The retro-psoas course of the common iliac artery is among the rarest of vascular anomalies, with fewer than 10 cases documented in the literature. This case is notable not only for the retro-psoas common iliac course but for the accompanying constellation of ipsilateral anomalies, including an absent internal iliac artery, a tortuous and positionally inverted external iliac artery, and a ureteral course that follows the vein rather than the artery. Although the findings were incidental and the patient asymptomatic at the time of discovery, the anatomic complexity has meaningful implications for any future surgical or endovascular intervention. Preoperative vascular mapping with dedicated CTA or conventional angiography may be beneficial.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2026;Online ahead of publication
Publication date:
June 24, 2026
Author Affiliations:
1. Medical Student, Oakland University William Beaumont School of Medicine Rochester, Michigan, USA
2. Diagnostic Radiology, Corewell Health William Beaumont University Hospital, Royal Oak, Michigan, USA
Corresponding author:
Matthew Tufts
Medical Student, Oakland University William Beaumont School of Medicine
586 Pioneer Dr, Rochester, Michigan 48309, USA
Email: [email protected]


")

")

