ORIGINAL RESEARCH
Arterial assessment of the lower limb and foot: perceived benefits and disadvantages of current methods in contemporary practice
Doyle KJ,1 Levy NF,2 Atkin L,3,4 Ousey KJ,3* Childs C1
Plain English Summary
Why we undertook the work: Many people have poor blood supply to the legs, which is known as peripheral arterial disease (PAD). This has a burden both for the patient and for healthcare services. It is important that assessments are used to make sure people have the right care at the right time. There are a range of tests used by healthcare professionals to assess and diagnose PAD. We wanted to explore what tests were used and what health practitioners thought about them. This was to help think about what devices might be useful in the future to help, or even to improve, PAD assessment.
What we did: An electronic survey was sent out to healthcare professionals asking them what assessments they used, how easy these were to complete, how long it took them and if there were any problems with completing them.
What we found: The survey was completed by 247 people. The largest group to complete the survey were podiatrists followed by community nurses, tissue viability nurses, vascular nurses, doctors and lymphoedema nurses. Manual assessments were most often used for measuring ankle and arm blood pressure to understand how healthy a patient’s blood supply to the legs was. However, there were some difficulties in assessing patients. This was due to broken equipment, lack of equipment, lack of training or patient health issues. Patient health issues included being unable to lie flat, having very swollen lower legs, or the assessment causing pain, meaning it could not be completed.
What this means: Future technology to assess lower limb circulation could be improved. Alternative systems could be developed to improve assessment of the circulation in patients with PAD.
Abstract
Background: Peripheral artery disease (PAD) is a subtype of atherosclerotic cardiovascular disease, most commonly affecting arteries of the lower limb. PAD brings a significant burden to healthcare systems. This paper presents the results of a cross-sectional survey investigating current practices and perceptions surrounding vascular assessment performed by healthcare practitioners in community and acute care. An online survey using several social media channels, professional societies and personal networks was distributed for a nominal period of 3 months.
Methods: Responses were received from 247 practitioners working in community and hospital settings across Great Britain and Northern Ireland. The largest group were podiatrists followed by community nurses, tissue viability nurses, vascular nurses and doctors. Practitioners frequently undertook assessments at multiple locations. Taking vascular assessments were part of their daily (n=151, 61%) or weekly (n=62, 25%) role. For the remainder, assessments were made less regularly; monthly (n=23, 9%) or rarely (n=10, 4%). Several systems were in use for vascular assessment, the majority manually operated.
Results: Across the range of instrumentation used, numerous equipment issues were reported. Of 390 stated problems, Doppler probe malfunction/casing breakage (n=160, 41%) was the most common followed by flat batteries (n=134, 34%), problems with arm and ankle cuffs (n=54, 14%) and burst toe pressure cuffs (n=24, 6%). Other issues included loose wires, faulty electronics, tubing detachment from cuffs and loss of waveform. Practitioners frequently employed multiple methods of vascular assessment. Of the 247 respondents, ankle-brachial pressure index was used by the majority (n=194, 79%), whilst toe pressure measurements for calculating toe-brachial pressure index were used by 109 (44%). Numerous barriers were identified in performing assessments: lack of time, lack of equipment, lack of training and lack of confidence. Participants also reported patient-based barriers including lack of patient mobility to lie supine, lower limb oedema and discomfort during assessment. It may be prudent for future technologies to consider alternative assessment methods to prevent limitations of assessment on those with swollen, calcified and broken friable tissue and for those who are unable to lie in a supine position without experiencing discomfort and pain.
Conclusion: Based on the results of this work, there is justification to pursue development of novel technologies which, in the future, would make it easier for healthcare practitioners to assess lower limb and foot circulation with ease, greater accuracy and at lower cost to the NHS.
Introduction
Cardiovascular disease (CVD) is now a major public health concern and World Health Organisation (WHO) sustainable development goal (SDG).1 As a non-communicable disease, the SDG target is mortality reduction and prevention of disease burden (SDG 3.4.1).2 Arterial disease outside the brain or heart is referred to as peripheral artery disease (PAD), a subtype of atherosclerotic CVD, most commonly affecting arteries of the lower limb.3
Considering the significant burden that PAD brings to healthcare systems in both higher income countries and lower to middle income countries, efforts to meet WHO SDG 3.4 will only be achieved with prompt diagnosis. However, given that the spectrum of disease is wide, including people who are symptomatic and asymptomatic,4 there are reported concerns about the reliability, availability and use of current devices and methods for vascular assessment in PAD, especially in those patients with end-stage disease, chronic limb threatening ischaemia.5
PAD diagnosis is made upon a full lower limb vascular assessment including assessment of distal pulse and measurement of arterial pressure combined with symptom presentation.6 A common method of assessing arterial pressure is the calculation of the ankle-brachial pressure index (ABPI). This involves taking systolic pressure at the ankle (posterior tibial and dorsalis pedis) and dividing the reading by the highest systolic brachial pressure. Differences are reported as a ratio. In addition, more recent practice also extends to measurement of toe pressures and the corresponding toe-brachial pressure index (TBPI). Now, with the appearance of automated systems on the market, an understanding of contemporary measurement methods, techniques, instrumentation and procedures in use across Great Britain and Northern Ireland is warranted. The aim of the study therefore was to undertake an online survey seeking to better understand current practice as well as possibilities for technology development for those involved in the care of patients with lower limb circulatory disease.
Methods
This work was undertaken as part of a larger study funded by the Medical Research Council (MRC). Institutional ethics approval was obtained before commencing the study.
Study design and target audience
A cross-sectional survey was carried out to investigate current practices and perceptions surrounding vascular assessment performed by professional healthcare practitioners in community and acute care.
Questionnaire development
All authors contributed to the design of the questionnaire by drawing on their collective professional experiences in nursing, medicine, podiatry, community and acute care vascular assessment. The goal was to capture quantitative and qualitative data on a wide range of practice, knowledge levels and challenges encountered in everyday clinical settings. The questionnaire was distributed using free online software, Google Forms, chosen for its user-friendly interface and easy distribution.
Consent and confidentiality
Before accessing the survey questions, participants were presented with an information page outlining the study purpose, the voluntary nature of participation, and assurances regarding data confidentiality. Informed consent was implied by the participant decisions to proceed with the survey and by agreeing to an explicit statement of consent. No personal identifiers were collected. All responses were automatically anonymised upon submission.
Survey distribution and data collection
The survey link was distributed via several channels:
• Email invitations to professional societies including the Society of Tissue Viability, Society of Vascular Nurses as well as individual/collective contacts identified by the research team (eg, the Sheffield-wide community nursing teams and NHS vascular nurses).
• Announcements by specialist publisher Wounds UK (survey posted 19 September 2024) or newsletters where possible through established professional connections as well as social media streams such as ‘X’ (formerly known as Twitter) and closed Facebook groups related to peripheral artery disease or lower limb wounds.
• Personal networks of the co-authors (in collaboration with colleagues) – for example, podiatrists working within high-risk areas within the NHS – to further extend the reach.
• A time-limited window for data collection (nominally 3 months) was set to complete the questionnaire.
Data management and analysis
Submitted responses were stored securely in a password-protected online university repository. Upon closure of the survey, responses were exported to an Excel™ spreadsheet. All analyses were conducted at an aggregate level to maintain anonymity. Not all survey questions were answered by every individual. Open-ended survey responses such as those focused on barriers to vascular assessment and the role of PAD assessment were individually analysed by all the researchers with conceptual coding7 before being drawn together and consensus reached upon the data findings. Group level results are reported as well as anonymous quotations considered helpful to clarify content.
To balance accuracy with readability, percentages have been rounded to the nearest whole number where appropriate. Values of 0.5 and above have been rounded up, while those of 0.4 and below have been rounded down. As a result, percentage totals may not always equal exactly 100%.
Results
Respondents
The survey was open from 17 September to 12 November 2024. During the first 10 days 168 responses were received, followed by a further 79 over the remaining 47 days, resulting in a total of 247 completed questionnaires. Of these, 245 respondents provided location data. The majority were based in England (n=216, 88%), with 13 responses each from Wales and Scotland (5% each), and three from Northern Ireland (1%).
Practitioners
Of the 247 healthcare respondents working across community and hospital settings, the largest group were podiatrists (n=115, 47%). Others included community nurses (n=49, 20%), tissue viability nurses (n=29, 12%), vascular nurses (n=28, 11%) and doctors (physicians and surgeons) (n=17, 7%). Lymphoedema nurses also participated (n=4, 2%). An additional five (2%) selected the ‘other’ category, which included roles such as vascular scientist, exercise physiologist and assistant practitioner.
Time working as a healthcare professional ranged from 1 to >40 years. Of the 246 who provided service data, 56 (23%) had 1–9 years of experience and an almost equal number (n=62, 25%) had been practising for 10–19 years. A further 70 (28%) reported 20–29 years of experience, while 46 (19%) had worked for 30–39 years. Twelve (5%) had been practising for >40 years.
Among the 244 who provided educational information, the majority held a graduate level qualification (n=215, 88%). Of these, 84 (39%) had obtained a Master’s degree or Doctorate. The remaining respondents were educated to Diploma level or held other forms of certification (n=29, 12%).
Of the 246 who provided working sector data, the majority were employed exclusively within the NHS (n=195, 79%). A further group worked solely in the private sector (n=12, 5%) and the remainder combined NHS roles with other activities such as education, research or private practice.
Assessment locations
Practitioners frequently undertook assessments at multiple locations. The most frequently reported location was clinic-based practice (n=211, 85%), followed by domiciliary or community settings (n=138, 56%) as well as hospital wards (n=99, 40%). Less common settings included in a University, General Practice surgery or nursing home (n=3, 1%). Of the 247 respondents, 246 indicated that performing vascular assessments was a regular component of their professional responsibilities, with 151 (61%) undertaking them daily and 62 (25%) on a weekly basis. A smaller proportion reported conducting assessments less frequently, either monthly (n=23, 9%) or rarely (n=10, 4%). Several systems were in use for vascular assessment, the majority manually operated but automated systems were being used in everyday practice (Table 1).
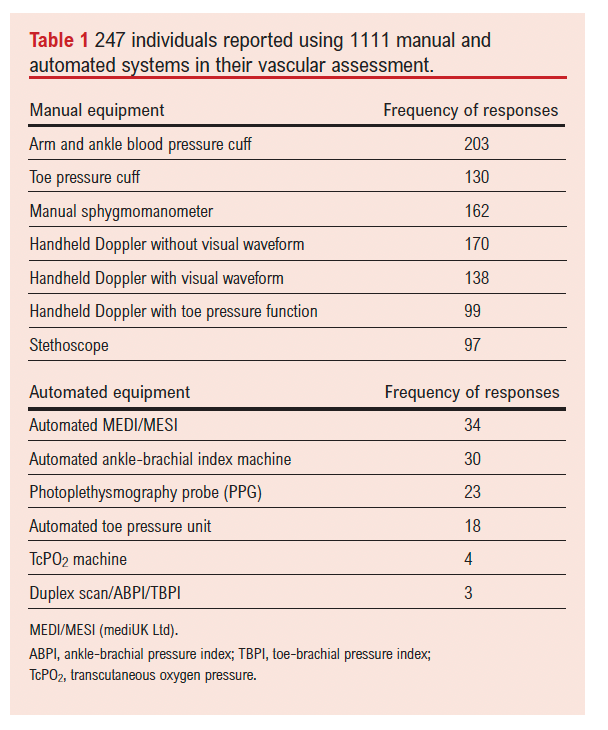
Huntleigh (Huntleigh Healthcare Ltd, Cardiff, UK) equipment was the most common supplier of vascular devices (including arm and ankle pressure cuffs), although practitioners reported using more than one type of vascular assessment device (eg, manual and automated systems) (Table 2).
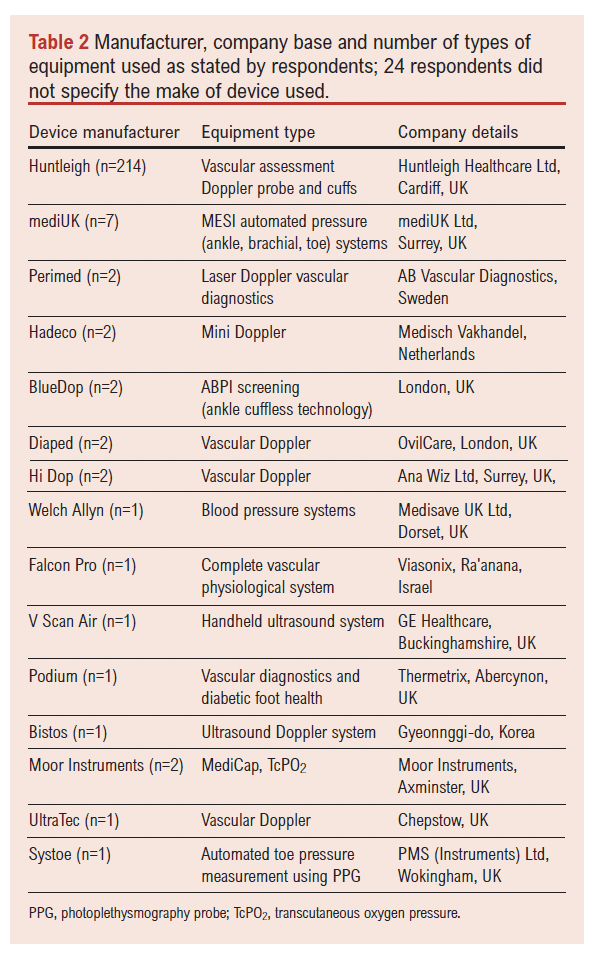
Multiple devices are in use in current practice for arterial pressures at the ankle, toe and arm, either manually or by automated systems. Photoplethysmography (PPG) was used in vascular assessment practice, most frequently by podiatrists. More advanced diagnostic systems such as duplex ultrasound was used by consultant podiatrist/clinicians, Perimed AB vascular diagnostics (Sweden) by podiatrists and a vascular scientist. Falcon (Viasonix, Ra’anana, Israel) was used by vascular nurses. Medicap (Moor Instruments, Axminster, UK) transcutaneous oxygen monitoring was used by podiatrists and a doctor.
Across the range of instrumentation/devices used, numerous equipment-related issues were reported, totalling 390 problems from the majority of respondents (n=202). The most frequently cited issue was Doppler probe malfunction or casing breakage (n=160, 41%), followed by flat batteries (n=134, 34%), problems with arm and ankle cuffs (n=54, 14%) and burst toe pressure cuffs (n=24, 6%). An additional 18 (5%) included loose wires, faulty electronics, tubing detachment from cuffs and loss of waveform.
Pressure measurements
Of the 246 who provided data on brachial pressure measurement, the majority (n=192, 78%) reported using the highest value obtained from the right and left arm readings in practice. A smaller group (n=12, 5%) used the right arm for right-sided ABPIs and the left arm for left-sided ABPIs. Among the remaining respondents (n=4, 2%), alternative methods were used such as selecting the easiest arm to access or adapting to patient-specific factors (for example, when a cannula was in situ). Thirty-eight participants (15%) either did not measure brachial pressure or did not provide a response to the question.
Ankle-brachial pressure (ABP) and calculation of index (ABPI)
Of the 246 who described their vascular assessment practice, 37 (15%) reported not including an ABPI calculation in their assessments. Of the remaining 209 who did include ABPI, the majority (n=170, 81%) reported always taking measurements from both legs. A further group did so only sometimes (n=31, 15%), while a small number measured the leg suspected of disease only (n=8, 4%). Doppler signals (sounds and waveforms) are key to ABPI and TBPI assessment, and headphones can enhance auditory signal detection. Fourteen (6%) reported using headphones regularly and 56 (23%) used them sometimes. However, the majority (n=177, 72%) reported never using headphones in their practice.
The time required to complete ABP measurements and to calculate ABPI varied among respondents. Of 201 practitioners who reported the duration of their assessments, the majority (n=114, 57%) indicated it took less than 20 minutes. A further 42 (21%) reported durations of 20 to <30 minutes while 45 (22%) stated that the procedure took 30 minutes to >1 hour. Most (n=132, 65%) considered that they had sufficient time to complete ABPI, whilst the remainder reported either not having enough time or expressed a preference for more time to carry out the procedure.
Practitioner views on the ease of completing ABPI assessments were divided. Of the 208 who answered this question, 102 (49%) reported finding the procedure easy, while a similar number (n=100, 48%) described it as sometimes difficult. A small number (n=6, 3%) found ABPI assessments either difficult or very difficult. Reported challenges included difficulty finding pulses, patient discomfort, limited time or lack of staffing, and lack of experience. With regard to calculation of the index, almost all respondents (n=209, 98%) reported feeling confident to undertake the calculation.
Toe-brachial pressure (TBP) and calculation of index (TBPI)
Compared with the number of practitioners performing ABPI as part of their vascular assessment, far fewer reported including toe pressure measurements or calculating the TBPI. For the 132 who provided data on time taken, 102 (77%) completed pressure measurements and TBPI calculation in <20 minutes, including 38 who reported taking <5 minutes. The remaining 30 (23%) reported durations ranging from 20 to 60 minutes. When asked whether there was enough time to perform a TBPI in the same appointment after completing an ABPI, the majority (n=158, 65%) reported that they either did not have sufficient time or would prefer more time. By contrast, 35% indicated that they had enough time to complete both ABPI and TBPI.
For the 136 respondents who commented on the ease of performing TBPI measurements, 51 (38%) found the assessment easy. However, 73 (54%) found it sometimes difficult, while eight (6%) described it as difficult and four (3%) as very difficult. Of 225 respondents who provided data on patient positioning during ABPI and TBPI assessments, nearly all (n=222, 99%) reported being able to help patients achieve the correct position. Of these, 11 (5%) stated they could do so always, 148 (66%) mostly and 63 (28%) sometimes. Only three (1%) indicated that they had difficulty positioning their patients appropriately for the assessments.
Vascular assessment barriers
When given the opportunity to report perceived barriers to performing vascular assessments through an open-ended question, 242 provided feedback, generating 628 unique responses. Of these, 77 (32%) reported no barriers to assessment. Among the remaining 165 (68%), 13 distinct themes emerged. The most often cited barriers included time constraints or lack of service capacity (n=202), insufficient experience, knowledge or training to perform the tests (n=179), malfunctioning or unavailable equipment (n=79) and lack of managerial support (n=24). Additional themes included low patient engagement, lack of clinical support and limited professional interest in vascular assessment.
Diagnostic cut-offs for PAD
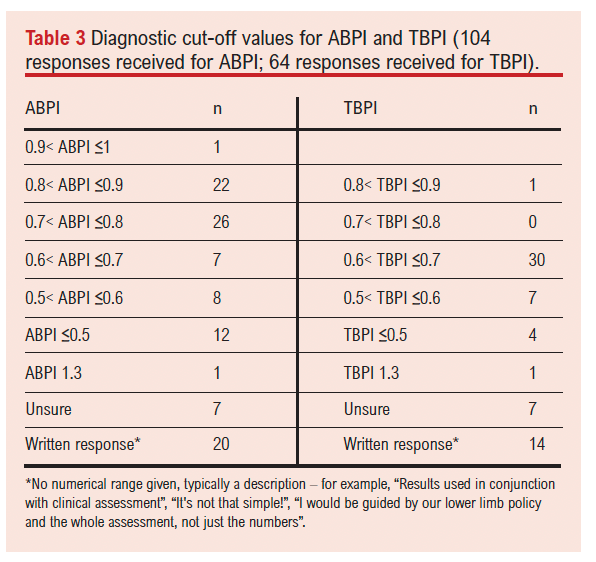
A variety of index test thresholds were in use in practice for both ABPI and TBPI. For ABPI, the most widely used was a threshold of >0.7 to <0.8 and, for TBPI, >0.6 to <7 (Table 3).
PAD screening
For the 184 who answered this question, the vast majority (n=172, 93%) believed that vascular assessments have a role in the preventative screening of PAD. Only 12 (7%) disagreed. Those in support of preventative screening highlighted benefits such as early detection of disease, the potential to prevent progression and the opportunity to manage risk factors proactively. Common themes included: “it would help detect disease earlier”, “prevent disease progression, because time is very important in PAD”, and “it would encourage early management and control of risk factors”. Others emphasised broader public health benefits, suggesting that the general public should be screened, and noting that “if PAD can be detected earlier, I believe treatment can be cheaper, with better prognosis” and “GPs should have capacity to perform ABPI”.
General perspectives from participants
Assessment opportunities and timing
There were areas of good supportive practices with respondents saying that they ran PAD triage clinics to detect early PAD, redirecting referrals from vascular surgeons to podiatry leg community-based services. “We have 60-minute appointments for these people +30 min administration time to cover assessment, diagnosis, breaking news, education about long term conditions and negotiation about BMI and lifestyle changes. Another stated, “All patients receive ABPI assessment within two weeks of admission to caseload”. On the other hand, there were comments indicating that respondents were concerned about lack of experience and time availability to be able to undertake the assessments, “Time and experience is the factor that holds back good assessments” and “A thorough assessment is not possible in the community, with the lack of equipment, time constraints and lack of exposure given, to be confident and competent in then relaying our findings with any confidence!”
Perceptions of equipment
“The kit falling apart is a disaster….”. Better functioning equipment goes in tandem with concerns for space and staff: “We need more resources i.e. better functioning equipment, clinic space, well trained staff” as well as a lack of equipment: “We use very basic vascular assessment” and “We have equipment but limited ABPI and TBPI machines ….”
Training, skill, experience and confidence in understanding results
A common theme was that there needs to be an increase in access to education about the assessments and for upskilling of staff to ensure confidence in the interpretation of results.
“The assessment itself is clear on what is required. The challenge lies with (a) interpretation of the results for clinicians who are not as skilled and/or do not feel competent in their assessment, and (b) patient impact and their presentation”.
“It is something that we can get comfortable with and better at with time and practice, there is sadly a lack of support with some of the technicalities with the equipment”.
“There needs to be major education”.
Clear guidance on when to refer to vascular services
It was thought that the ideal situation would be to have the assessments completed more frequently and regularly for patients with none or very minor symptoms, almost similar to screening, rather than assessments happening because the patients have advanced disease, but currently this was not feasible due to lack of education, skills and time constraints.
Many respondents felt the main problem was delayed referrals to the assessment service with concerns that, due to GP collectives, patients with lower limb wounds are referred to the acute sector: “Primary care practitioners no longer deal with wound care/active wounds, never mind prevention. Who is going to fund a program for preventative screening for PAD?! Great idea but unrealistic”.
Responses highlighted concerns surrounding those patients who are housebound: “My patients are all housebound, not able to get ongoing clinical support when there is doubt or a problem in doing test or interpreting results”.
Who should be undertaking assessments
Many respondents were keen for all practice staff to be educated in taking the assessments: “Would benefit from all staff in the treatment rooms being able to do toe pressures” and respondents who worked in podiatry settings stated: “ABPI needs to be encouraged to be performed routinely by all podiatry staff band 5+ not just specialist podiatrists”. Some respondents believed it was a simple process in a very easy patient but, if trying to make good referrals, accuracy and context was needed. As such, the assessment should be undertaken by a qualified podiatrist and should not be treated as a simple technical role for assistants. Others thought the role of specialists was key to good quality tests: “In secondary care the vascular scientist performs these tests and has a huge amount of learning background and training to achieve reliable readings”.
Emerging and automated systems for vascular assessment
New technologies used in vascular assessment arising primarily from research suggest that there is good support for their use in disease prognosis “TcP02 has been a game changer – we can assess chances of healing before toe amputation so know if we need to look at vascular intervention first. Saving money by reducing need for unnecessary imaging”. There was also support for the newer automated pressure systems but with recognition of the need for systems validation. “We also use automated assessments (MESI and BlueDop) but in a research capacity as there is a lack of data on the validity of these devices” “We would love to use blue dop or automated systems if safe”.
Follow-up monitoring
Continued monitoring was identified as a concern with a lack of time and staff capable of undertaking follow-up. Respondents stated that when they needed to refer to vascular (eg, due to unclear results and for safe compression) it could take a long time for patients to be seen and in the meantime ulcers and oedema were worsening. “In our lymphoedema clinic all new patients get a vascular assessment including ABPI or TBPI, but for ongoing monitoring purposes we would do the vascular assessment without the ABPI/TBPI; eg, the problems come on discharge, because we don’t have anyone to refer to for repeat vascular assessments”.
Discussion
In this survey we have attempted to understand the perspectives and experiences of frontline healthcare professionals in contemporary vascular assessment practice. Both positive and negative responses help towards healthcare improvement as well as facilitating the drive for MedTech development if there are technology gaps to close. A wide audience involved in all aspects of vascular assessment was reached whether practice was based in hospital, community or clinics. Linking with professional networks and societies focused on wound healing and vascular disease, 247 respondents submitted survey information about their day-to-day practice in under 2 months. With the survey design used, respondents were at liberty to provide information as a mix of discrete options as well as open-ended responses. This meant that response numbers varied between questions.
ABPI was by far the most common method for vascular assessment, with just over half taking toe pressure measurements for calculation of TBPI. Use of these assessment techniques is higher than those identified previously in UK-based studies. For example, 26% of 260 podiatrists were reported to perform ABPI and just 6% TBPI.8 A slightly higher percentage of activity was reported, with 32% of 307 podiatrists completing ABPI and a similar number (6%) completing TBPI.9 It is possible that, by moving from a single profession audience (podiatry) to a broader group of vascular practitioners, a wider perspective has been achieved where assessments are being performed involving ABPI and TBPI in day-to-day vascular care and treatment, than for podiatry where the nature of the specialty differs.
The higher rates of ABPI and TBPI assessments reported in the current survey may indicate a shift in practice consequent on publication of research (as well as national guideline recommendations for vascular assessment) after the previous surveys had been completed and published. Emphasis, particularly on the importance of ABPI in PAD assessment,10 may have resulted in greater recognition of the guidance translated to practice.
Non-invasive simple methods for disease detection in clinical practice are attractive, but tests need to be sufficiently reliable to prevent missed diagnoses. ABPI, as an index test for PAD with a threshold of <0.9, is recommended as the best predictor.11 This threshold has been used to distinguish positive (<0.90) and negative (>0.90) ABPI test results.12 When referring to guidelines, clinicians use this threshold in practice. However, false negative and false positive test results do occur.13 This is recognised as a confounder to test accuracy, especially when used for lower limb PAD in patients with medial artery calcification at the ankle arising from incompressible tibial vessels. This is a common finding in patients with diabetes who present with symptoms of PAD and foot ulcers,14-16 making ABPI a significant limitation when used for vascular assessment in diabetic patients. With increasing rates of diabetes in the community,17,18 diagnostic accuracy is key to early intervention and treatment. Of concern here is diagnostic performance of ABPI against gold standard angiography, with sensitivity for PAD diagnosis ranging widely.19 For example, a high level of specificity (83.3–99.0%) for an ABPI <0.90 was reported, but with a wide range of sensitivity (15–79%).20 Low sensitivity, especially in older people and those with diabetes, was also noted.20 Some confusion may exist about the relationship between guidelines for PAD diagnosis and venous disease, where ABPI is used as a safety check for strong compression therapy.21 Safe compression is indicated when ABPI is >0.8 in venous disease and is the mainstay of treatment in those with venous leg ulcers. This subtle detail in knowledge of the respective ABPI thresholds could sometimes be misinterpreted by lower limb clinicians, especially those in the leg ulcer management field. For those with end-stage PAD presenting as chronic limb threatening ischaemia, it has been noted that partial compression of the vessel may underestimate the severity of the disease.22 In a large series of nearly 6,000 patients undergoing revascularisation, 21% had a ‘normal’ ABPI and 53% had a mild reduction in ABPI only, indicating a ‘disconnect’ in the utility of ABPI in certain populations of patients.22
Whilst expert consensus recommends toe pressures and TBPI for its advantages over ABPI23 in the presence of heavily calcified tibial vessels, there still lacks an agreement on the threshold.24 Furthermore, a threshold for TBPI (and toe pressure) to confirm diagnosis does not exist.5 Even so, just over half of respondents were using TBPI in their practice with the majority using a threshold of 0.7, where TBPI >0.7 indicates that diagnosis of PAD is less likely.24
Whilst the greater number of respondents in the survey measure ABPI and/or TBPI manually, a smaller group have adopted automated monitoring, despite recommendations that such systems to detect PAD in people with leg ulcers should be used only in the context of research.25,26 This may be due to previous evidence of poor diagnostic precision comparing manual with automated systems for measuring ABPI (sensitivity 75%, specificity 67%).27
Focusing on barriers to performing vascular assessments, 628 open comments were received. Thematic analysis of the open questions identified barriers falling into 14 themes, of which four were key – namely, lack of time, lack of equipment, lack of experience training and confidence. The lower percentage of practitioners completing TBPI assessment may reflect a lack of training and confidence with toe pressure assessment. Comments from participants repeatedly reported upon TBPI being a ‘faff’ or ‘fiddly’. Less experienced clinicians reported uncertainty in the assembly of the equipment and lack of confidence with interpreting the readings. There was a clear commentary on the necessity for additional training to enhance skills to help provide confidence on correct equipment use. In a systematic review, ABPI education was explored.28 It was concluded that training requires time, mentorship and feedback on all stages of the ABPI procedure. To date, there is no standardised training to close these training gaps, suggesting that some patients may be receiving suboptimal assessment, falling short of recommendations and guidance by national and international health agencies.24,29 This background is mirrored to an extent by the issues arising in this survey, where lack of training, lack of confidence and a recognition of the need to upskill staff was repeatedly identified as an area of concern.
Focusing on patient-based barriers to performing vascular assessments, open responses identified key themes – namely, lack of patient mobility to lie supine, limb oedema and discomfort during assessment. These findings are comparable to those identified in a study exploring PPG versus ABPI assessment in patients with PAD.30 The feedback from this survey identified factors such as inability to lie flat as a barrier to ABPI assessment and discomfort or pain on cuff inflation at the ankle. It is clear that neither ABPI nor TBPI is suitable for all patients, at all times, who require assessment for PAD. Newer technologies may be more suitable. However, results from the current survey identify little use of alternative technologies that do not rely on cuff inflation, with only 23 respondents using PPG for example. It may be prudent for future technologies to consider alterative assessment methods to prevent limitation of assessment on those with swollen, calcified and broken friable tissue and for those who are unable to lie in a supine position without experiencing discomfort and pain.
Conclusion
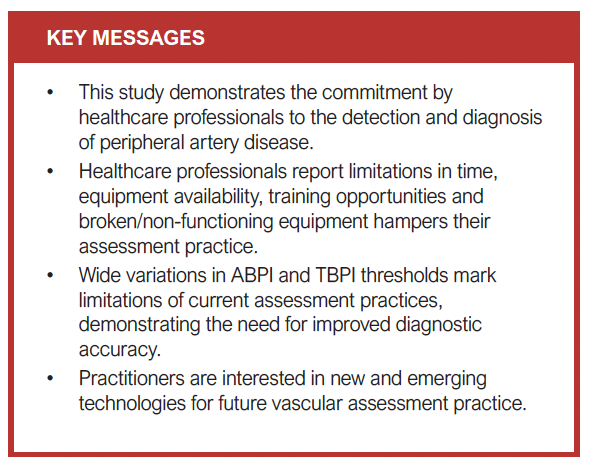
This national survey has provided an important insight into the current practices, experiences and challenges associated with lower limb vascular assessment in clinical practice across Great Britain and Northern Ireland. The findings demonstrate a clear commitment by healthcare professionals to the detection and diagnosis of PAD, with high levels of engagement in ABPI assessments and, to a lesser extent, TBPI measurements. Despite improvements compared with earlier surveys, particularly in the uptake of ABPI and TBPI, significant barriers persist. These include limitations in time, equipment availability, clinician training and confidence, and patient-specific factors such as discomfort, immobility and advanced disease presentation.
Notably, the variation in diagnostic thresholds used in practice, along with confusion between national guidelines, indicates a need for clearer and more unified clinical guidance. This, combined with persistent uncertainty around TBPI thresholds and limitations of ABPI in certain populations, underscores the necessity for improved diagnostic accuracy through both enhanced clinician education and the development of validated user-friendly technologies.
The limited adoption of emerging and automated technologies, despite practitioner interest, further highlights a critical area for future development. This includes the potential value of technologies not dependent on cuff inflation and more adaptable to the needs of patients with complex presentations. If PAD is to be diagnosed earlier and more accurately, particularly in community settings, investment in both workforce training and technology is essential. Ultimately, achieving the WHO sustainable development goal2 of reducing mortality from non-communicable diseases will require a coordinated response that addresses systemic barriers, improves diagnostic reliability and enables equitable access to high-quality vascular assessment across all care settings.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2025;4(4):190-198
Publication date:
August 18, 2025
Author Affiliations:
1. Health Research Institute, Centre for Applied Health and Social Care Research, Sheffield Hallam University, Sheffield, UK
2. Department of Podiatry, University of Huddersfield, Huddersfield, UK
3. Institute for Skin Integrity and Infection Prevention, University of Huddersfield, Huddersfield, UK
4. Mid Yorkshire NHS Teaching Trust, Wakefield, UK
*Currently Professor Emeritus and Clinical Manager (wounds), Omniamed Communications
Corresponding author:
Professor Charmaine Childs Health Research Institute, Collegiate Campus, Sheffield Hallam University, Broomhall Road, Sheffield S10 2BP, UK
Email: [email protected]


")

")

