ORIGINAL RESEARCH
Calculating and reducing the environmental impact of hybrid endovascular surgery
Sharma Y,1 DawsonT,2 Motta A,3 Patel A,1,3 Garnham A,4,5 Sandford B1,3
Plain English Summary
Why we undertook the work: Healthcare creates lots of greenhouse gases and surgery plays a big role in this. Surgical cases require a lot of disposable single-use equipment, anaesthetic gases and high-energy systems like ventilation, lighting and temperature control. This study measured the carbon footprint of common arterial vascular surgeries and explored ways to reduce their environmental impact.
What we did: At one vascular surgery centre we studied four types of vascular surgery procedures: simple endovascular (keyhole) aneurysm repair (EVAR); complex EVAR (involving custom-made devices and extra branches for arteries to the internal organs); percutaneous (keyhole) lower limb procedures for circulation like angioplasty and stents; and hybrid lower limb revascularisation involving a combination of open surgery and keyhole procedures. For each operation we recorded in real time the devices, disposable items and waste produced. We then estimated the carbon emissions associated with each item by considering its full journey from producing the raw materials and manufacturing the product through to packaging and transport and finally disposal. This approach, known as a life-cycle assessment, looks at the environmental impact of a product from when it is made to when it is thrown away.
What we found: The amount of carbon emissions varied depending on the type of procedure. Complex EVAR had the highest average carbon emissions since it uses more resources and is more complicated. This was about the same as driving 418 miles in a petrol-driven car. We also saw that more people in the operating theatre resulted in a greater number of single-use wearable items such as hats and gowns being used, adding to the waste produced. Ways to reduce the emissions could include using more keyhole techniques, reusable surgical fabrics, ecofriendly packaging and more efficient imaging methods.
What this means: This study is the first to look at the carbon footprint of common arterial vascular surgeries and identifies where changes could be made to make these procedures more environmentally friendly. As this study is an early exploratory investigation, further research involving multiple hospitals and a wider range of procedures is needed to confirm these findings and to see whether these changes really make surgery more environmentally friendly.
Abstract
Background: The healthcare sector is a substantial contributor to global greenhouse gas emissions, with surgical services accounting for a significant proportion. This is driven by the extensive use of single-use consumables, volatile anaesthetic agents and energy-intensive infrastructure including ventilation, lighting and climate control systems. This study quantified the carbon footprint of commonly performed arterial vascular procedures and identified modifiable drivers to reduce their environmental impact.
Methods: A prospective observational study was carried out at a single vascular surgery centre, focusing on four procedure types: simple endovascular aneurysm repair (EVAR); complex EVAR; percutaneous lower limb revascularisation; and hybrid lower limb revascularisation. Real-time data were collected to capture devices, consumables and waste associated with each intervention. A life-cycle assessment approach was used to estimate carbon emissions across the product pathway including raw material extraction, manufacturing, packaging, transportation and disposal.
Results: A total of 24 procedures were analysed (6 simple EVAR, 8 complex EVAR, 5 percutaneous lower limb revascularisations and 5 hybrid lower limb revascularisations). Carbon emissions varied significantly between procedure types (Kruskal–Wallis test, H=11.53, p<0.05), with complex EVAR associated with the highest median emissions, reflecting greater resource intensity and procedural complexity. Median emissions for complex EVAR were equivalent to driving approximately 418 miles in a standard petrol vehicle. A strong positive correlation was seen between the number of theatre personnel and the volume of single-use wearable items (Spearman’s ρ=0.878, p<0.001), suggesting staffing levels contribute meaningfully to procedural waste. Opportunities to reduce emissions were identified, including use of percutaneous techniques, reusable surgical textiles, sustainable packaging strategies and imaging optimisation.
Conclusion: This pilot study represents the first observational quantification of the carbon footprint associated with common arterial vascular procedures and identifies targets for sustainability interventions within vascular surgery. Given the procedural heterogeneity and single-centre design, further multicentre studies with larger sample sizes and standardised methodologies are required to better quantify emissions and evaluate the effectiveness of sustainability interventions.
Introduction
Background
Climate change refers to long-term shifts in global temperatures and weather patterns, driven predominantly over the past two centuries by human activity, particularly the combustion of fossil fuels. The release of greenhouse gases such as carbon dioxide (CO2) and methane (CH4) traps heat within the atmosphere, raising global temperatures,1 which is known as global warming. This represents one of the prime manifestations of climate change, alongside air pollution, increase in prevalence of human diseases, food insecurity and other socioeconomic impacts. Climate change has escalated into a global emergency, affecting ecosystems, economies and public health worldwide.
The Paris Agreement, signed in 2016, aimed to limit the global mean temperature rise to below 2°C and to achieve net negative emissions by 2100. However, current projections suggest that, even with immediate action, global temperatures are expected to continue rising by an additional 0.2–0.5°C over the next decade, potentially reaching a 1°C increase by the end of the 21st century. The World Health Organization (WHO) has projected that climate change will cause 250,000 additional deaths between 2030 and 2050, with the burden of climate change not being distributed equally. Vulnerable communities face disproportionate health risks due to limited access to well-resourced healthcare and food security systems.2 This highlights the critical need for stronger and more unified global mitigation efforts to effectively combat climate change.3
Climate change and healthcare
The increasing contribution of healthcare systems4 to the global climate emergency is now widely recognised. The global health sector was estimated to generate 2.6 billion metric tonnes of carbon dioxide equivalent (CO2e) in 2011, and in 2014 the global health climate footprint accounted for approximately 4.4% of total global emissions, equivalent to the greenhouse gas emissions from 514 coal-fired power plants.5
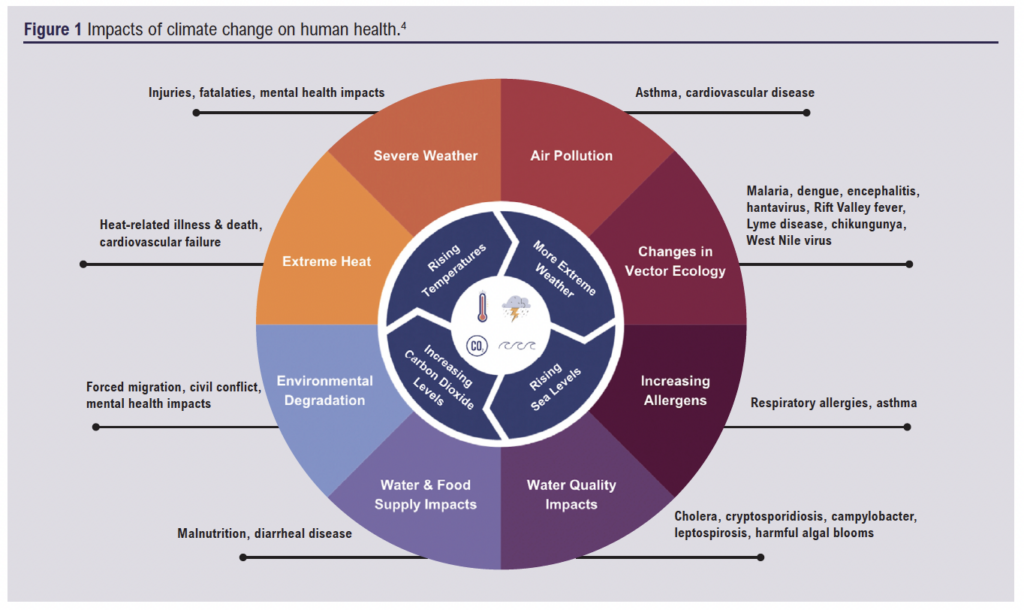
The increase in greenhouse gas emissions and the resulting intensification of the climate crisis presents both direct and indirect risks to public health. These risks include injury, illness from changes to vector ecology, air pollution and natural disasters (Figure 1). This creates a cycle in which worsening climate-related health outcomes increase healthcare demand, further amplifying healthcare-related emissions. As this cycle continues the burden on healthcare systems grows, making it increasingly challenging to mitigate both climate-related health issues and the environmental impact of healthcare systems.4
Recognising the environmental responsibility, the NHS set an aim to become the world’s first net zero national health service. The plan outlines two key targets: achieving net zero for the NHS Carbon Footprint by 2040 (covering emissions under direct control) and net zero for the NHS Carbon Footprint Plus by 2045, which includes emissions from the supply chain, patient and staff travel, and commissioned services.6
Surgery and sustainability
Within healthcare, surgical care has been identified as a significant contributor to the global climate emergency due to the extensive use of energy, medical devices and consumables and generation of waste. The energy performance of the surgical suite at John Radcliffe Hospital was shown to be 12.61 GJ/m2 compared with 2.14 GJ/m2 for the building as a whole, demonstrating the increased energy intensity of operating theatres.7 A systematic review which aimed to determine the reported carbon footprints of surgical operations in hospitals worldwide identified medical devices and consumables to be the greatest contributor to their carbon footprints (Figure 2), most likely due to their increased requirement in surgery to ensure sterility and efficiency.
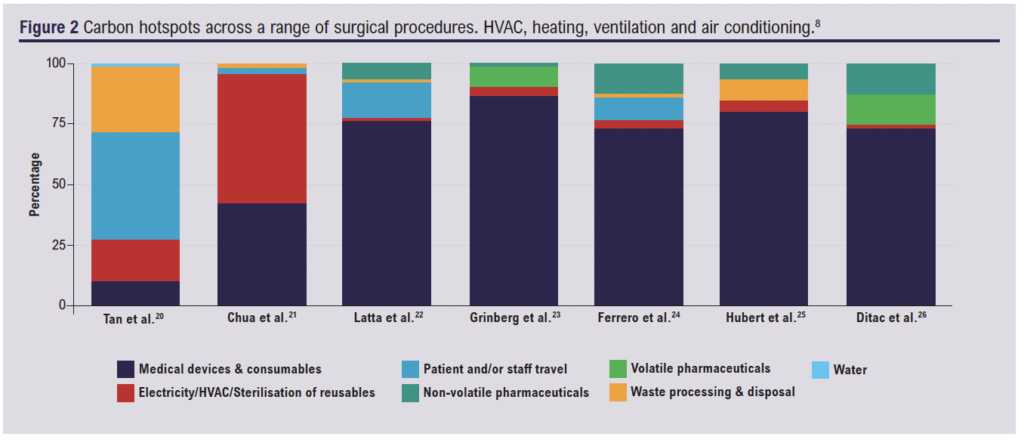
Carbon footprint contribution deriving from transportation of these medical devices and consumables makes up only a small proportion of the total carbon footprint, therefore attempts at reducing the carbon footprint should be focused on other areas. The material production and manufacture of medical devices and consumables was the greatest contributor of their emissions and highlights an area in which more sustainable alternatives could be used, such as through the substitution of single-use items with reusable types. An essential detail which emerges from systematic reviews conducted to determine the reported carbon footprint of surgical operations is that there are no specific guidelines for calculating the carbon footprint of surgical operations, causing diverse results between studies. Standardisation of methods will provide better quality data in order to guide more sustainable surgical practice.8
Vascular surgery and sustainability
Vascular surgery is a unique surgical specialty in that open surgery, endovascular interventions and hybrid techniques are all used in the management of life- and limb-threatening conditions. Endovascular surgery has evolved rapidly over the last 50 years as evidence of reduced periprocedural morbidity and mortality compared with open surgery emerged.9 Hybrid techniques incorporating elements of both open and endovascular surgery are now common. These procedures have become the standard of care for many patients with life- and limb-threatening ischaemia, and guidelines from major clinical bodies such as the National Institute for Health and Care Excellence (NICE) and the European Society for Vascular Surgery (ESVS) increasingly recommend endovascular interventions as the preferred approach for treating abdominal aortic aneurysms.10,11
Endovascular surgical techniques call for specialised equipment such as guidewires, angiographic catheters, balloons and stents, all of which are composed of complex synthetic materials such as polytetrafluoroethylene (PTFE), teflon, stainless steel and nitinol, which increase their cost and environmental impact (polyethylene is more affordable and more environmentally friendly than PTFE, yet PTFE is still more commonly used12).13 The packaging associated with these devices is also extensive. One study on packaging materials associated with equipment used in endovascular aneurysm repair (EVAR), a common vascular surgical procedure, found that typical equipment packaging contained between four and seven elements to hold one device, such as cardboard or plastic inserts, foam and sterility packaging. Some of these packaging items lack the universal recyclable symbol, causing uncertainty of their disposable methods even though the majority of materials were classed as recyclable when discussed with company representatives. The shift towards minimally invasive procedures has led to greater reliance on these disposable devices in vascular surgery, and a formal framework to mitigate the environmental impact of vascular surgery is needed.14
A few studies have quantified the carbon footprint of vascular procedures, Gu et al15 showed that the median amount of carbon produced over 59 vascular procedures was 15.2 kg CO2e, roughly equivalent to driving a car for 108 km.16 Many vascular and endovascular procedures are difficult to fully standardise and therefore few studies have attempted to assess arterial interventions. Notably, a recent study by Sénémaud et al17 evaluated the carbon footprint associated with a single EVAR, estimating it to generate a median of 108 kg of CO2e and identifying consumables to be one of the most emissive factors. More specific evidence on the environmental impact of vascular surgery remains limited and, as endovascular techniques continue to grow, their collective environmental impact will likely increase, highlighting the need for robust data in order to develop effective tools to reduce their environmental impact.
Aims and objectives
The primary aim of this study was to describe the environmental impact of commonly performed arterial vascular procedures. With a particular focus on carbon emissions generated through the use of disposable medical devices and consumables and waste management, the study sought to address a critical gap in the existing literature.
The secondary aim was to assess the potential for carbon footprint reduction through changes in clinical practice, such as the adoption of reusable surgical textiles and reusable instrument sets. By assessing the environmental implications of such changes, this study aims to provide practical recommendations for transitioning towards more sustainable surgical practices.
The specific objectives guiding the study to achieve these aims are:
1. To systematically identify and document the equipment used in common arterial vascular procedures and to analyse the associated waste disposal practices, including the classification and management of different waste streams.
2. To calculate the carbon footprint of commonly performed arterial vascular procedures by integrating observational data with life-cycle methodology, published manufacturer-derived data, online sources and published emission factors.
3. To estimate the potential environmental cost savings associated with change in clinical practice, with a particular focus on substitution of single-use surgical textiles with reusable textiles.
Methods
Study design
In this observational exploratory pilot study, prospective data collection methods were employed to assess the environmental impact of commonly performed vascular surgical procedures. A life-cycle assessment (LCA) was used to estimate the carbon footprint associated with disposable medical devices and equipment used.
The LCA focused on per-procedure resource use rather than top-down economic input-output modelling, allowing attribution of emissions to specific items and waste streams used during individual cases. An LCA is a standardised approach used to evaluate the environmental impact of a product or process across its entire life-cycle, from raw material extraction and manufacturing, use, their associated packaging and disposal practices, measured in kilograms of CO2 equivalent (kg CO2e). In this context, it enables the identification of carbon intensive components and supports evidence-based changes to more sustainable clinical practice.18 This study primarily employed a bottom-up, process-based LCA using per-procedure resource use data collected in real time. Where item-specific life-cycle data were unavailable, top-down published emission factors were applied for material production, transport and waste processing.
This study was conducted with local audit approval (project no. 16785).
Procedure selection
Four procedures were selected as follows:
1. Standard endovascular aneurysm repair (EVAR), which is defined as any EVAR procedure using a standard infrarenal device (stent graft) following the manufacturer’s instructions, without the use of any adjunctive procedures.
2. Complex endovascular aneurysm repair (complex EVAR), defined as any EVAR procedure that includes fenestrated, branched, customised or internal iliac branch devices.
3. Percutaneous lower limb intervention, referring to a range of minimally invasive procedures performed to manage peripheral arterial disease, particularly in cases of chronic limb- threatening ischaemia. The procedures aim to revascularise occluded or stenotic arteries (ie, percutaneous transluminal angioplasty (PTA) and stenting).
4. Hybrid lower limb revascularisation, a combined approach which integrates both open and endovascular techniques to revascularise in patients with complex peripheral arterial disease (eg, common femoral endarterectomy alongside endovascular treatment of the iliac, superficial femoral or tibial arteries).
The four selected procedures are among the most commonly performed vascular procedures in the UK, with approximately 43,000 vascular surgery procedures being carried out in England each year and more than 28,000 of those cases relating to aortic aneurysm repair and lower limb revascularisation. There has been an increase in endovascular procedures in recent years as techniques such as EVAR have been established,19 with lower patient mortality and morbidity,20 increasing the patient population eligible for treatment.
These procedures are widely recognised and recommended for treatment for different manifestations of arterial disease and chronic limb-threatening ischaemia by various guidelines such as the NICE, the ESVS and the Trans-Atlantic Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II).10,20,21
As such, they are being increasingly favoured over purely open strategies and will remain highly relevant in clinical practice. As these procedures become more common, and the complexity of interventions achievable with endovascular and hybrid techniques increases, the collective carbon footprint will also increase, making it essential to understand and reduce environmental impacts through developing sustainable practices.
Four operative groups were included in this study as described above, with consecutive cases being recorded where a data collector was available. There were no specific exclusion criteria, although the hybrid peripheral revascularisation group referred specifically to the hybrid nature of the revascularisation, rather than a purely endovascular procedure combined with adjunctive minor amputation.
Data collection
Data collection was performed by a single operator (YS) over a two-month period, during which 28 cases were selected and observed. A case was observed from the time the patient entered the operating room from the anaesthetic room, until the patient exited for the recovery ward. Data regarding the following were recorded: personal protective equipment (such as gloves and masks), surgical fabrics (such as drapes and gowns), implantable and single-use devices and consumables, all packaging materials associated with devices and consumables, waste produced from the procedure, and data on reusable items. A database of all medical devices, disposables, reusable items, packaging and waste of observed cases was constructed.
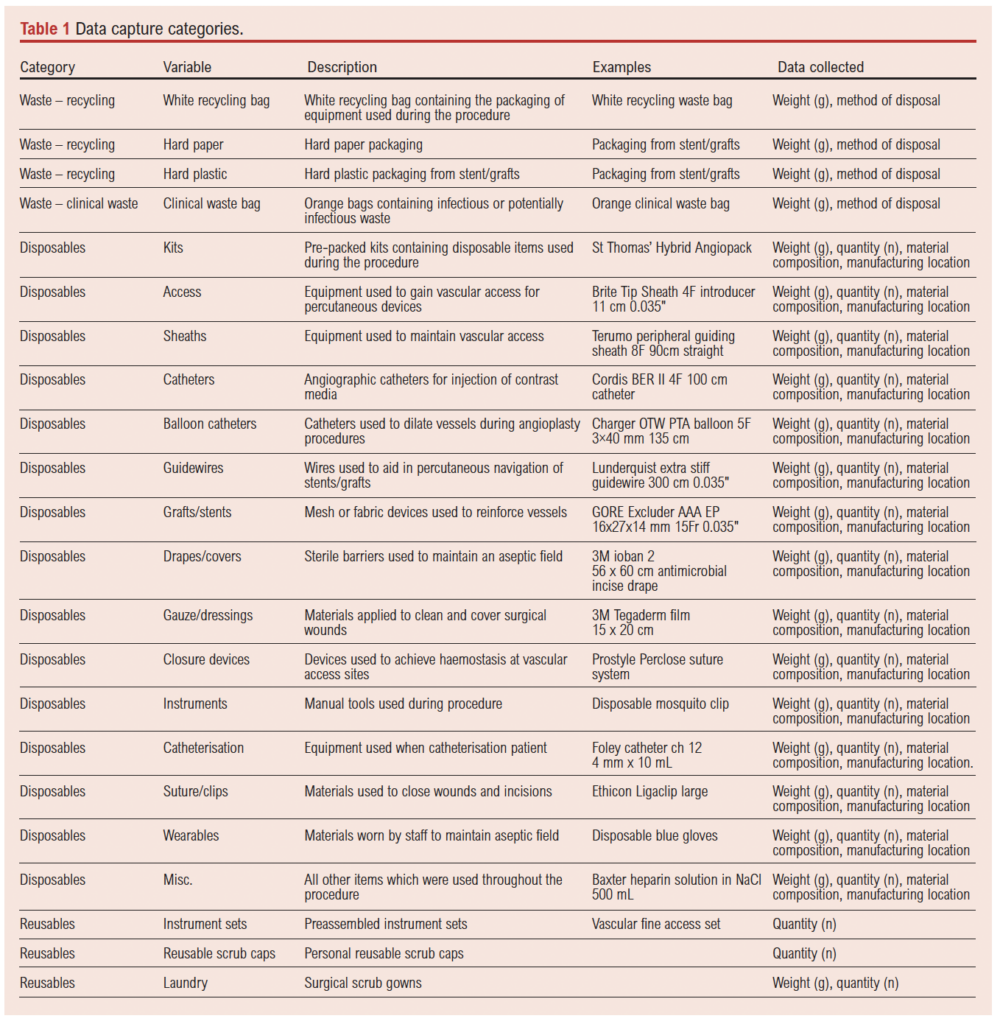
Data regarding devices such as catheters, guidewires, stent grafts and consumables, such as gloves and gowns, included the product type, the total weight of the item and the weight of the corresponding packaging, the quantity used, the manufacturing location of the item and the main material composition of the product and its packaging. Data regarding devices and consumables that had been opened but not used would also be recorded. The category ‘miscellaneous disposables’ included individual single-use items not captured within predefined device categories including syringes, labels, caps, connectors and other small ancillary materials used during routine procedural workflow. The waste produced from each procedure was categorised as recycling – which itself comprised white recycling bag waste and hard plastic and paper kept aside separately for recycling – and clinical waste, which was then weighed. Methods of waste management such as incineration and recycling were also recorded. Data regarding reusable items and laundry recorded the quantity, category (eg, reusable scrub gowns, reusable instrument sets/kits) and weight, referring to sterile instrument sets assembled and packaged locally within the hospital sterile services department, containing reusable procedural instruments prepared for specific vascular interventions. These sets did not include disposable consumables and were recorded separately from single-use items (Table 1).
All weights were recorded using a DIGI® DS-502 weighing scale (maximum capacity 6 kg) to the nearest gram, with no individual item exceeding this limit, and the database for data collection was constructed on Microsoft Excel™. Data on manufacturing location and material composition of disposable medical equipment were gathered by examining the labelling and manufacturing details printed on the product packaging where available, but when such details were not clearly specified, data were gathered through online searches including manufacturing websites, product brochures and other publicly available online sources. The data on identifying waste streams and their associated carbon emissions with their respective disposal methods were obtained through direct correspondence with the trust waste manager of Guy’s and St Thomas’ NHS Foundation Trust. All the data were collected through direct observation in the hybrid theatre at St Thomas’ Hospital, and all appropriate cases during the time period were to be observed, accepting limitations around time commitments for a single data observer.
Data analysis and LCA calculations
Categorical data, such as quantity of disposables were presented as numbers and percentages, and continuous data such as the total carbon footprint per type of procedure were described using inclusive median and interquartile range (IQR). Planned statistical analyses included non-parametric comparisons between procedure groups (Kruksall–Wallis tests) and correlation analyses (Spearman’s rank correlation). The clinical-to-recycling waste ratio was calculated for each case by dividing the weight of clinical waste by the weight of the recyclable waste produced. The total carbon footprint for each case was quantified using Formula 1 (see Appendix 1 online at www.jvsgbi.com).
The CO2e associated with disposable items was estimated using a process-based LCA approach, combining measured item weights with emission factors to account for raw material production, manufacturing, packaging, transport, and end-of-life waste processing, allowing the contribution of each stage to the total carbon footprint to be understood, meaning that carbon saving strategies can easily be applied to stages which contribute the most. The LCA calculator used for this study is shown in Formula 2 (see Appendix 1 online at www.jvsgbi.com).
The CO2e from raw material processing of disposables was quantified by identifying the main material components and using respective emission factors obtained from online sources, discussed in (see Appendix 2 online at www.jvsgbi.com). Transport CO2e was calculated by identifying the manufacturing location, and then using a publicly available online sea shipping route calculator22 to obtain the distance to St Thomas’ Hospital, London, in kilometres, covering both sea and road distances. Subsequently, the emission factors for shipping through general sea and road freight obtained from the greenhouse gas reporting conversion factors 2024 spreadsheet from the Department for Energy Security and Net Zero were used to calculate the CO2e.23 The contribution of CO2e from end-of-life treatment was obtained by using emission factors provided by the trust waste manager of Guy’s and St Thomas’ NHS Foundation Trust, with the emission factors for waste processing differing between recycling and clinical waste with 359 kg CO2e produced for processing one tonne of clinical waste compared with 21 kg CO2e /tonne for recycling processes (Guy’s and St Thomas’ NHS Foundation Trust Waste Management Team).
In the absence of published item-specific life-cycle data for manufacturing and packaging stages, a simplified mass-based emission factor of 0.001 kg CO2e per gram (equivalent to 1 kg CO2e per kg of material) was applied. This value was selected as a screening-level approximation and applied consistently across all items to enable comparative analysis between procedures within this exploratory pilot study. Mass-based proxy emission factors were used where item-specific data were unavailable, consistent with ISO 14040 guidance permitting the use of representative secondary data within life-cycle inventory analysis provided assumptions and limitations are transparently reported. Published LCAs of plastics manufacturing report supply chain emission intensities typically within the order of approximately 1–5 kg CO2e per kg of material, placing the selected value within the lower range of empirically reported estimates for polymer manufacturing.24
More granular proportional attribution using material-specific emission factors (eg, DEFRA conversion factors for plastics, paper, and cardboard packaging) was not undertaken in this pilot analysis in order to maintain methodological consistency across heterogeneous devices and packaging types. Introducing variable material-specific factors without complete component standardisation may have introduced additional uncertainty and reduced comparability between procedures. However, incorporation of such approaches represents an important refinement for future work.
Maintaining a uniform modelling approach across all procedures ensured internal consistency of emission estimates, allowing relative differences between procedure types to be interpreted with greater confidence within this exploratory pilot framework.
The CO2e from laundry is relevant due to the use of reusable surgical gowns. However, it should be noted that centre-specific emission factors were not obtainable, so instead emission factors deriving from a LCA of items commonly reprocessed by a large hospital laundry service were used.25
In each case the ‘St Thomas’ Hybrid Angio Pack’ refers to a pre-packaged set of disposable items consisting of 44 individual items including drapes, hypodermic needles, disposable plastic kidney dishes, galley pots, etc. The above carbon emissions calculator formula has been applied to these items, resulting in a total CO2e per ‘St Thomas’ Hybrid Angio Pack’ of 46.1 kg CO2e (see Appendix 3 online at www.jvsgbi.com). This has then been included as a single item for subsequent descriptive statistics.
For each case, pre-filled bags of heparinised saline solution (heparin sodium 1000 units/500 mL infusion Viaflex bags) were utilised.26 The CO2e calculations for this were generated based on the above LCA calculator, by taking the heparin additive into account for the carbon emissions deriving from raw material processing, which is not synthetic but extracted from animal-based materials (porcine intestinal mucosa).26 To estimate the carbon emissions, published data were used which indicated that the rearing of a single pig produces approximately 670 kg CO2e, and each pig yields approximately 65,000 IU of heparin,27 therefore the carbon emissions deriving from a 1000 IU dose was able to be calculated by substituting the following variable into Formula 3 (see Appendix 1 online at www.jvsgbi.com).
Assumptions
Several assumptions were made during the data analysis process, due to lack of data being publicly available and to ensure consistency. Medical devices and equipment are made of several individual components, using a variety of materials. The use of patents and trademarks by manufacturers limits the data available in the public domain, and therefore material composition was limited to the two most predominant materials, estimated using publicly available online resources and through the use of open-source AI.
The use of a simplified mass-based emission factor for manufacturing and packaging and attribution based on dominant material compositions represents a screening- level approximation. Incorporation of material-specific emission factors and full component inventories may refine absolute emission estimates but is unlikely to substantially alter relative comparisons between procedure groups.
For CO2e relating to transport, once the manufacturing location was identified (once again estimates had to be made when specific details were not available, such as if a country of manufacture was provided, the capital city of that country was used as the manufacturing location), it was entered into an online shipping route calculator, using St Thomas’ Hospital as the destination in order to calculate the total distance by road and sea shipping, with sea shipping routes that use the London Gateway Port as the point of entry into the UK for consistency across data. It was assumed that container ships with an average TEU and diesel HGV trucks which where average laden were used for sea and road transport.
Centre-specific emission factors for the sterilisation of reusable instrument kits were not able to be obtained and therefore were excluded from the total carbon footprint. However, the contribution of sterilisation of single-use items has previously been estimated at <1%.28 Similarly, for the purposes of this study, anaesthetic components of care, which have been well described in the existing literature,29 were excluded as were staff and patient travel, hospital infrastructure and out of theatre patient care components. These elements have all been previously studied30 and fall outside the remit of this study, given the time limitations. There is unlikely to be significant variation in these elements for this study compared with the previously published data.
Results
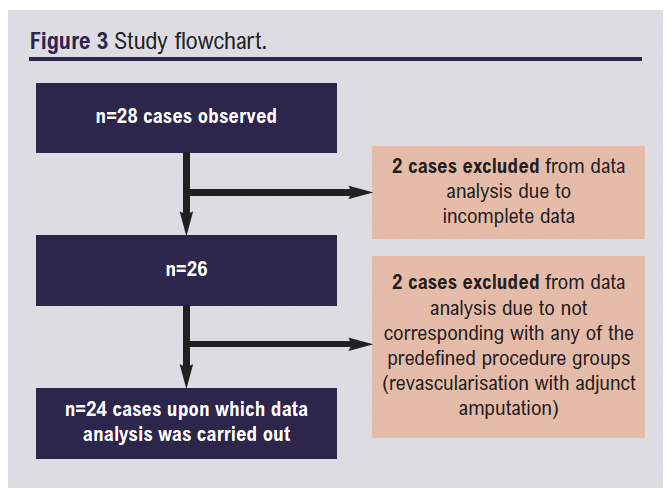
A total of 28 cases were observed, with the previously mentioned data analysis methodologies only being applied to 24 of them. The flowchart in Figure 3 illustrates the process. These consisted of simple EVAR (n=6), complex EVAR (n=8), percutaneous lower limb revascularisation (n=5) and hybrid lower limb revascularisation (n=5).
Disposable item analysis
For each of the procedure types studied the number of disposable items used is shown in Table 2, giving the median (IQR) number of items for each procedure type due to the small sample sizes and non-normal distributions observed across procedure groups.
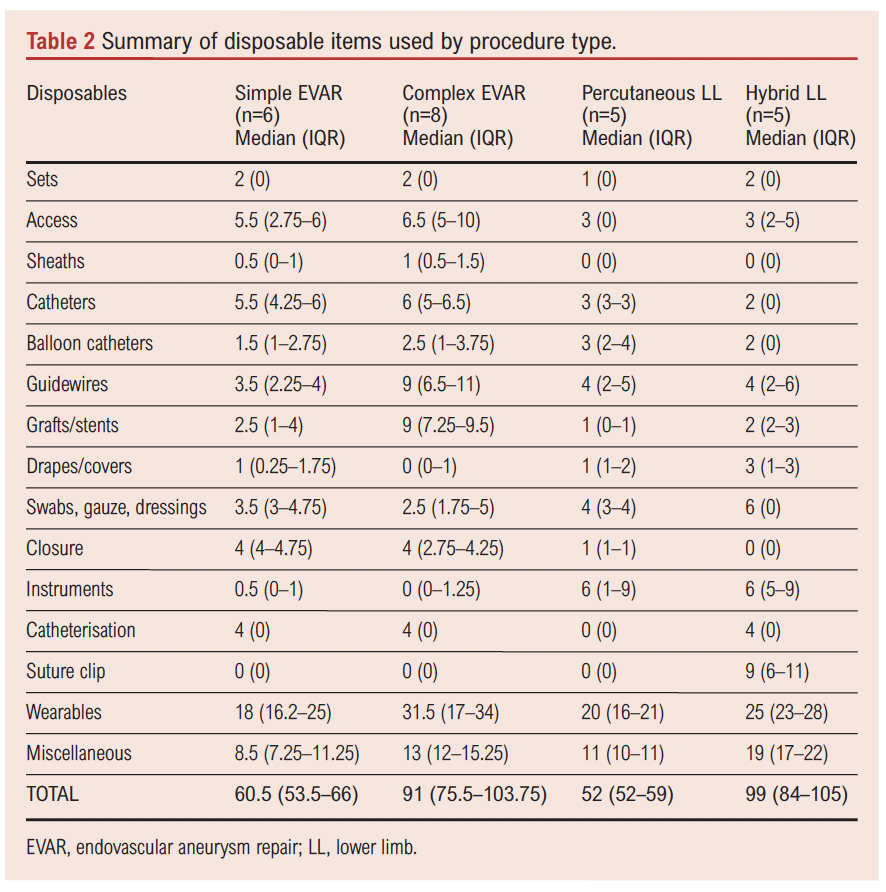
The data showed variation between cases and groups, with the complexity of the case having a direct correlation with the number of disposables. The median (IQR) number of disposable items used per procedure was 70.5 (58.5–97). When stratified by procedure type, hybrid lower limb revascularisation procedures showed the highest number of disposables used (99 (84–105)), followed by complex EVAR procedures (91 (75.5–103.75)), simple EVAR (60.5 (53.5–66)) and percutaneous lower limb interventions (52 (52–59)).
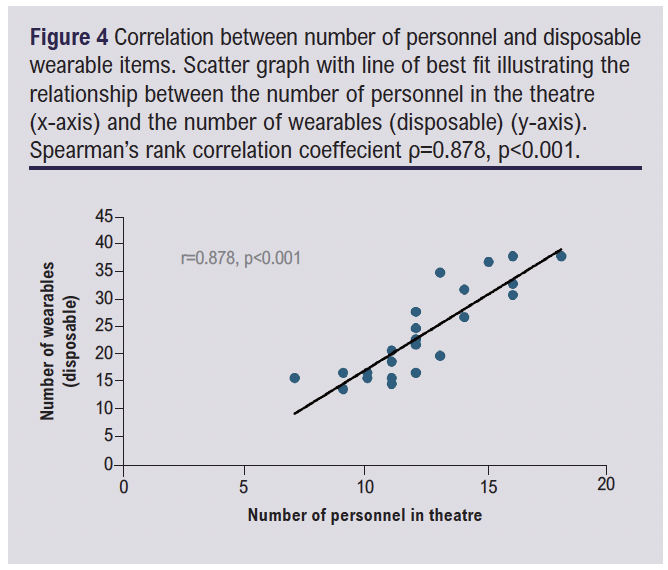
More personnel were present during complex procedures, which correlated with a greater number of wearable disposable items used during the case (Figure 4). Spearman’s rank correlation coefficient was selected as a non-parametric method to assess the association between these two variables. The analysis confirmed a strong positive correlation between the two variables (Spearman’s ρ=0.878, p<0.001). These findings are consistent with expectations, as each theatre personnel requires disposable items to maintain sterility, and the significance of the observed relationship emphasises the impact that personnel numbers may have on the overall carbon footprint.
Waste generation analysis
The median waste generated per case also varied between procedure types. The weight of waste is given to the nearest gram. Separate analysis of recyclable waste and clinical waste is given in Figures 5 and 6.
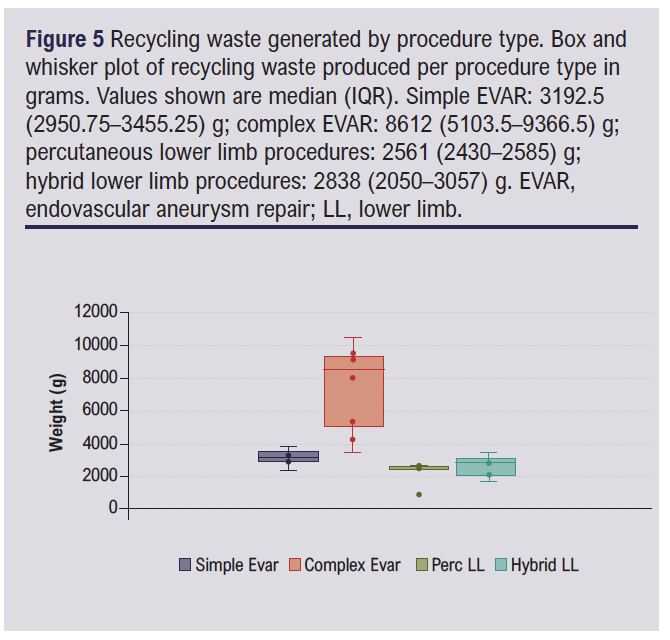
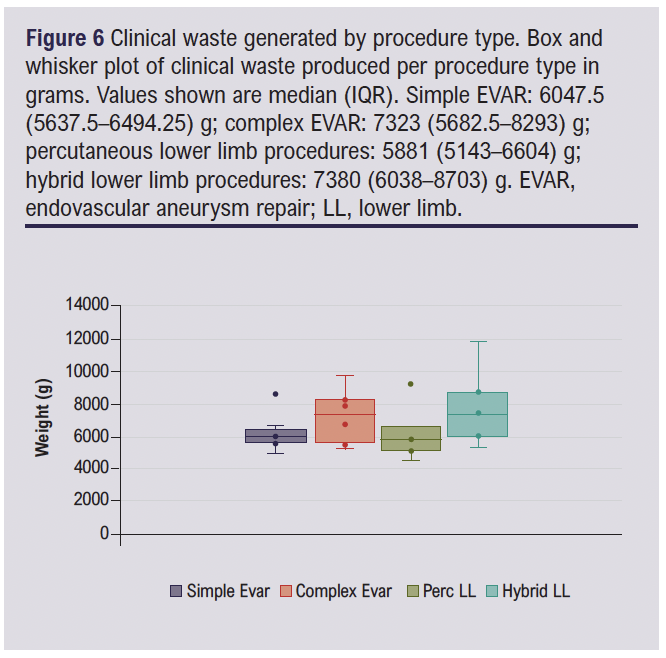
Differences in both clinical waste and recyclable waste were noted across groups with the complex EVAR and hybrid lower limb revascularisation groups again representing the greater waste generation.
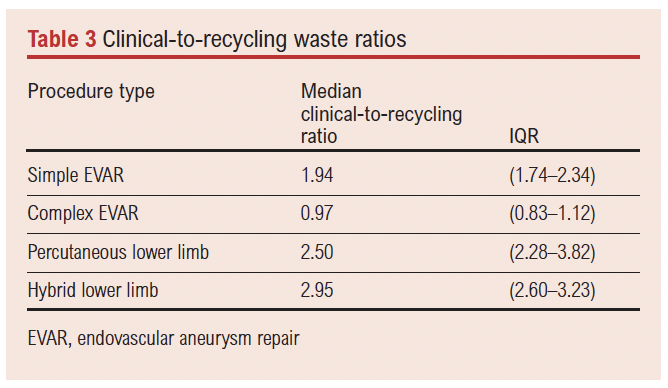
A Kruskal–Wallis test was performed to determine if there were statistically significant differences in the clinical-to-recycling waste ratios across procedure types. This statistical test was selected as it is a non-parametric method for comparing continuous non-normally distributed data across multiple independent groups. The analysis showed a significant difference between groups (H=18.09, p=0.00042), indicating that the proportion of clinical waste to recycled waste differed between procedure types. The median clinical-to-recycling waste ratios varied between procedure types (Table 3), suggesting that hybrid and percutaneous lower limb procedures tended to generate proportionally greater amounts of clinical waste relative to recycling waste.
LCA results
LCA of carbon emissions of disposable items was conducted for each case. The full data tables are given in Appendix 3 (online at www.jvsgbi.com). Similar to the disposable items and waste analysis, the complex EVAR (median (IQR) 110.59 (100.77–121.87) kg CO2e) and hybrid lower limb revascularisation groups (median (IQR) 86.59 (70.56–94.70) kg CO2e) were the procedure groups generating the most carbon waste, and the complex EVAR group generated significantly greater CO2e than the hybrid lower limb revascularisation group (Figure 7).
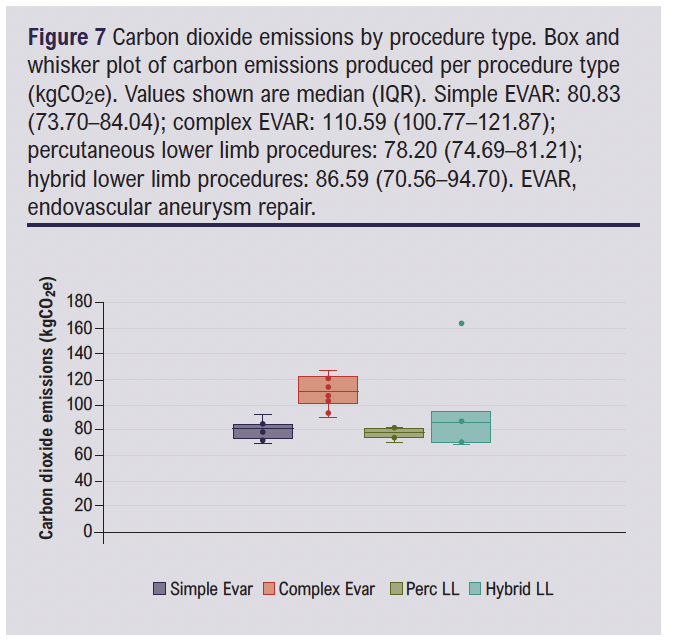
Another Kruskal–Wallis analysis demonstrated a significant difference in carbon emissions across the four procedure groups (H=11.53, p=0.0092), indicating that the environmental impact varied depending on the procedure type. It is likely that this relates to the greater complexity of the implantable devices used across groups, with complex EVAR cases requiring custom-made stent grafts and other specialised equipment, often involving more complex manufacturing processes and potentially greater shipping distances, although this subgroup analysis was beyond the scope of the current project.
The emission factor for laundry processing was obtained from published results from an LCA which aimed to estimate the environmental impact of linen items reprocessed by a large hospital laundry unit and was 0.508 kg CO2e per kg of laundry.25
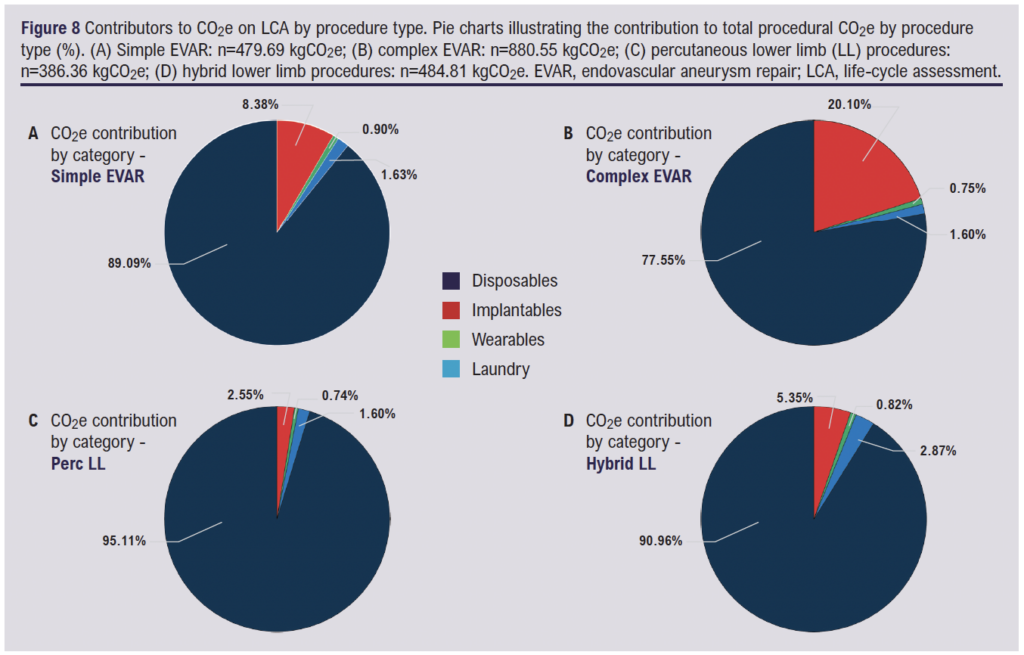
In order to investigate the contributors to CO2e generation, all emission-generating components which were used in the LCA calculations were further categorised into four categories: single-use disposables (sheaths, guidewires, catheters, balloon catheters, swabs/gauze/dressings, instruments, kits, drapes/covers, access and closure devices, equipment used when catheterising patients, suture/clips), implantable devices (stent/grafts), wearables (hats, masks, gloves, gowns) and laundry.
Analysis of CO2e contributions by components across the four procedure types revealed that single-use disposables were the predominant source of emissions in all cases, accounting for 77.55–95.11% of total procedure-related CO2e (Figure 8). The proportion attributable to disposables was highest in percutaneous lower limb interventions (95.11%) and lowest in complex EVAR cases (77.55%), in which a greater reliance on stents and grafts resulted in a higher relative contribution from implantables (20.10%). Implantables contributed minimally in simple EVAR (8.38%), hybrid lower limb (5.35%) and percutaneous lower limb (2.55%) procedures. Wearables and laundry represented minor emission sources overall, each contributing minimally across all procedure types. These findings indicate that disposables and implantable devices are the primary contributors to procedural carbon emissions, and targeted carbon-saving strategies should prioritise these domains to optimise sustainability in vascular surgical practice.
Discussion
This exploratory study aimed to estimate the carbon footprint associated with four common arterial endovascular surgical procedures. Through understanding the main procedural components to the environmental impact from surgery, it may be possible to reduce emissions through targeted system change. The main findings are that procedural carbon emissions varied by procedure type, with higher emissions observed in more complex endovascular and hybrid procedures, and that disposable medical devices and consumables accounted for the largest proportion of total emissions across all procedure types. Given the pilot nature of this study, these findings should be interpreted as descriptive. The study was designed to provide baseline data that may inform future sustainability research within vascular surgery.
The carbon emission data obtained from this study are likely to underestimate the actual carbon emissions for the procedures, as certain contributing factors were not included in the analysis such as energy use of the theatre as a whole, carbon emissions from anaesthesia and transport of staff and patients, based on existing literature and the pragmatic constraints of a pilot design. Operating theatres and hybrid suites vary widely in size, ventilation requirements, imaging capabilities and procedural duration is likely to differ between simple and complex interventions as well as between operators. These factors may meaningfully influence energy consumption and could vary by procedure type. Incorporating direct measurement or estimation of theatre energy use represents an important area for future research.
The total carbon footprint of a procedure would comprise all the emission-generating components, such as anaesthesia, for which there is also published literature. The anaesthetic team at Guy’s and St Thomas’ NHS Foundation Trust have moved away from inhaled volatile gas-based anaesthesia to total intravenous anaesthetic techniques, known to confer reduced carbon emissions.29 This is standard practice across all vascular anaesthetists and all procedure types, and therefore would have been unlikely to impact the results discussed in this study focusing on vascular surgery.
The study highlights differences in environmental impacts with each different procedure type. In particular, the clinical waste generation and total carbon emissions generated through complex hybrid lower limb revascularisations were high, and significantly greater than for percutaneous lower limb revascularisations. This is expected, given the hybrid nature of the intervention involving open common femoral surgery in addition to the endovascular components of the procedure.
Interestingly, although the complex EVAR group was the greatest contributor to overall carbon emissions, the clinical waste generation was low and emissions seemed to relate largely to graft manufacture and transport. Recyclable waste was high in this group, reflecting the large number of disposable and implantable items which are packaged in paper and plastic-based materials.
The findings of this study align with and expand upon previous work quantifying the environmental impact of surgical procedures. The study supports the findings of Rizan et al31 who identified single-use consumables and textiles as major contributors to surgical emissions. In particular, the high carbon emissions generated in complex endovascular and hybrid revascularisation procedures in this analysis reflect the intensive use of disposable equipment. While prior research has focused on general surgery, orthopaedics or anaesthetic-related emissions, this study adds to a growing body of evidence highlighting the high carbon intensity of device-heavy specialties such as vascular surgery. The waste generated per procedure observed here are consistent with ranges reported in studies of comparable surgical complexity such as arthroscopic procedures,32 and the carbon emissions generated and quantity of disposables are consistent with ranges reported from a previous study quantifying the carbon footprint of EVAR procedures.17
The data were collected through real-time observation of procedures, which allowed for a highly accurate documentation of devices and consumables used and waste produced. The direct observation allowed for the identification of different categories of waste like recycling and clinical waste and, by distinguishing between different waste streams, this study provides a greater understanding of their individual contributions to total carbon emissions. The prospective nature of the study meant that all data were documented accurately from the moment the patient entered the operating theatre to the moment of exit, including data on items which may not be listed on procedure logs or in inventory records, improving the accuracy of the dataset.
The use of a single observer for data collection allowed for a greater understanding of procedural practices. The nuances between theatre staff in their practices when setting up for procedures and waste management was able to be observed, ensuring that a standardised method was consistently applied when collecting data.
To the team’s knowledge, this is also the first study to explore the environmental impact of different vascular and endovascular arterial procedures and therefore generates new knowledge which may equip clinical teams with information necessary to consider systematic change towards greener vascular practice.
In capturing ‘real world’ complex cases rather than those more standardised and easily protocolised cases (eg, endovenous ablation), the study results are relevant and valid in relation to the varied and complex vascular cases which require operative intervention, providing information on which decisions can be made to reduce environmental impact.
Despite the strengths of this study, several limitations must be acknowledged when interpreting the findings. The heterogeneity within the dataset was a primary challenge. Variability arising from differences in procedure type and complexity and also the surgical practices of individual surgeons resulted in a wide variety in the quantity of consumables, which limits the generalisability of the findings. A larger dataset incorporating a broader range of procedures would be necessary to draw more statistically robust conclusions.
The study was conducted in a single centre, introducing further limitations due to variability in surgical practices across vascular units, waste management and procurement choices of equipment between trusts in the UK. A multicentre study would therefore be required to validate the findings and to ensure the results have a broader applicability across different geographic sites. The relatively small sample size also limits the conclusions which may be drawn from the results. The limited number of cases reduces statistical power to detect meaningful differences in CO2e.
Operator experience, procedural complexity and case duration are likely to influence resource utilisation and emissions; however, the sample size was insufficient to permit stratified analysis by operator type or experience. Future studies with larger cohorts may allow exploration of whether emissions vary systematically according to operator factors or procedural efficiency.
Manufacturers were not directly consulted regarding device transport pathways and shipment modes were estimated using standard assumptions. Variability in transport logistics, including potential use of air freight, may influence absolute emission estimates and represent an area for refinement in future analyses through industry collaboration.
Although having a single observer ensured a consistent approach to data collection, it also introduces the potential for bias. The presence of one observer may have influenced the behaviour of theatre staff, and the subjective judgement of the single observer may have caused data to be incorrectly categorised or recorded.
Opportunities to reduce environmental impact
Several opportunities to reduce the environmental impact of vascular surgical practice have been identified through this study and in the wider literature. A key intervention applicable across all procedure types is the transition from disposable to reusable surgical fabrics. Adoption of reusable textiles represents a simplified practical change, requiring minimal alteration to clinical workflows or staff training. A 2018 study by Vozzola et al33 showed that the use of reusable isolation gowns over disposable isolation gowns resulted in a 30% reduction in greenhouse gas emissions (kg CO2e). This reduction was largely attributed to decreased clinical waste generation and the elimination of repeated manufacturing processes associated with single-use gowns. The study also noted that reusable gowns could offer additional environmental benefits such as lower water and energy usage when processed through modern industrial-scale laundering systems, which often incorporate wastewater treatment facilities to reduce the environmental impact of water output from the cleaning process.
A more comprehensive follow-up study by the same group in 2020 focused specifically on surgical gowns and reported an even greater reduction in carbon emissions, up to 66% (kg CO2e), when using reusable gowns compared with disposables.34 This larger reduction compared with the 30% seen in the earlier isolation gown study is primarily attributable to differences in the type of gown assessed and the inclusion of more detailed life-cycle components in the analysis. Unlike the previous study, which focused on isolation gowns with limited packaging and fewer handling steps, the 2020 study evaluated surgical gowns which typically require more robust manufacturing, sterility controls and packaging. The analysis accounted for all stages from raw material extraction through to end-of-life disposal and included emissions from packaging production, the full energy demands of repeated laundering cycles and the role of wastewater treatment plants used in modern laundry systems. By incorporating these additional factors, particularly transport, industrial-scale cleaning infrastructure and textile processing, the study offered a more accurate estimation of the emissions associated with each gown type, thereby highlighting the substantial carbon savings achievable through reusable systems.
The findings from both studies reinforce the role of textile-related choices as a key area of opportunity for carbon emission reduction within surgical care. Although the exact scale of savings may vary depending on gown type, laundering system and hospital infrastructure, the consistent finding across multiple analyses is that reusable gowns lead to substantial and repeatable reductions in carbon emissions. At St Thomas’ Hospital reusable surgical gowns are already standard practice, representing a strong commitment to sustainable procurement. However, further environmental gains could be achieved by optimising elements of the laundering system, particularly through investment in more efficient wastewater treatment infrastructure to reduce the footprint of repeated washes. Additionally, while life cycle models often assume a defined reuse limit, typically 75 uses per gown, based on manufacturers’ advice, in practice, gowns at St Thomas’ are washed and reused indefinitely until failure, which may in fact amplify the carbon savings beyond those reported in the literature. This study did not assess infection risk or barrier performance associated with reusable surgical textiles, and conclusions regarding clinical safety cannot be drawn. The results reinforce the potential of reusable surgical textiles as a practical and impactful intervention to reduce the carbon footprint of routine surgical care.
The paradigm shift towards prioritising percutaneous lower limb revascularisation over hybrid lower limb procedures highlights a key clinical strategy in reducing the carbon footprint of vascular procedures. Full percutaneous techniques such as interventions at the common femoral artery have been shown to be increasingly effective, with low rates of periprocedural complications and mortality and better patency.35 By minimising the need for open surgical exposure, percutaneous approaches can decrease operative time, reduce consumable use and lower waste generation, all contributing to a lower procedural carbon footprint. However, it is essential that environmental consideration does not override clinical judgement. Decisions regarding revascularisation strategy should remain grounded in patient selection, anatomical suitability, risk stratification and multidisciplinary team discussion to ensure optimal clinical outcomes. Sustainability consideration may complement – but should not replace – established decision-making frameworks.
Packaging waste also represents a significant contributor to the total carbon footprint of surgical procedures, with medical consumables and devices being packaged in multiple layers to ensure sterility and prevent damage to fragile components. The widespread use of virgin plastics and complex composite materials – which are often trademarked and patented – reduce the recycling opportunities. Switching to biodegradable or recycled plastics offers a sustainable solution to this problem, but collaboration between healthcare institutes and industry partners is needed to encourage greener packaging practices and is a complex and time-consuming process.
A further opportunity identified for reducing procedural carbon emissions relates to imaging modality choices during vascular interventions. Digital subtraction angiography is commonly used in vascular procedures for its enhanced imaging quality; however, recent research has shown that this technique contributes significantly more to procedural carbon emissions compared with standard fluoroscopic imaging runs.36 Considering minimising the number of digital subtraction angiograms and using fluoroscopy where possible could potentially contribute to overall reduced CO2e per procedure without compromising patient safety, in addition to reducing procedural radiation exposure.
Conclusion
This exploratory study aimed to estimate the carbon footprint associated with four vascular surgical procedures, demonstrating that emissions vary by procedure type and are largely driven by disposable medical devices and consumables.
The findings from this study represent a small pilot single-centre investigation, but at the time of writing it is the first study to describe the environmental impacts of arterial vascular procedures commonly performed for life- and limb-threatening pathologies. The procedures represent a common subset of procedures used in clinical practice due to their minimally invasive nature and favourable patient outcomes, but their dependence on disposable devices and consumables presents a difficult environmental challenge.19
To address this environmental challenge, a multifaceted approach will be required, involving reduced reliance on disposables through increasing use of reusable textiles and instruments where possible, implementing better waste management protocols and collaborating with industry partners to promote the development of more sustainable devices and packaging.
Despite the limited scope of this study, the results highlight the significant carbon footprint generated by endovascular and hybrid techniques. These findings provide us with essential baseline data to build upon for future efforts aimed at reducing the environmental impact of vascular surgery, and future work is required to validate and consolidate the findings through larger multicentre studies with more comprehensive data collection.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2026;5(3):152-155
Publication date:
March 31, 2026
Author Affiliations:
1. King’s College London, London, UK
2. University of Exeter, Exeter, UK
3. Guy’s and St Thomas’ NHS Trust, London, UK
4. Royal Wolverhampton NHS Trust, Wolverhampton, UK
5. West Midland Deanery, Birmingham, UK
Corresponding author:
Becky Sandford
Vascular and Endovascular Surgeon, Guy’s and St Thomas’ NHS Trust, Honorary Senior Lecturer, King’s College London, Academic Department of Surgery, Level 1 North Wing, St Thomas’ Hospital, Westminster Bridge Road, London SE1 7EH, UK
Email: [email protected]


")

")

