CASE REPORT
Giant aneurysm of the dorsalis pedis artery: a rare pathology
Gunawardena T
Abstract
True aneurysms of the dorsalis pedis artery are extremely rare. This case report describes a 53-year-old male patient who presented with a rapidly enlarging pulsatile lump at the dorsum of his right foot. Imaging studies confirmed this to be a true aneurysm of the dorsalis pedis artery. As the large lesion was causing functional impairment, operative repair was offered. The aneurysm was excised and the arterial continuity was restored with a saphenous vein interposition graft. This case report aims to highlight this rare pathology and management considerations.
Introduction
Aneurysms of the foot arteries are rare.1,2 The majority of such lesions are post-traumatic false aneurysms. In contrast, true aneurysms that contain all three layers of the arterial wall are less frequently encountered.2-4 Such aneurysms have the potential for complications due to thrombosis or embolism.5 Unlike true aneurysms of the abdominal aorta, popliteal artery or major visceral arteries which have clearly established management guidelines, there is no consensus on when to intervene for these lesions.1 Here we report a patient who underwent open repair of a true dorsalis pedis artery (DPA) aneurysm with a reversed greater saphenous vein (GSV) interposition graft.
Case report
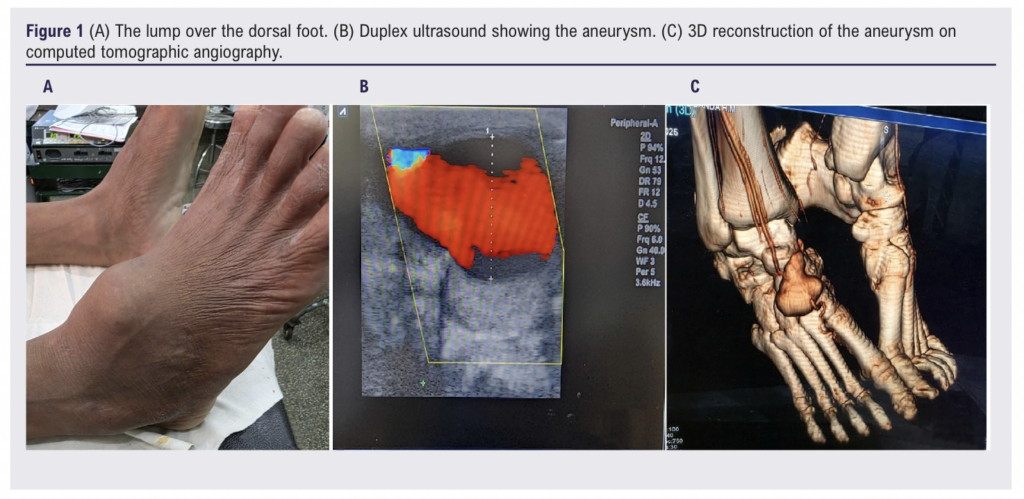
A 53-year-old previously well male presented with a painless but rapidly enlarging lump over the dorsal aspect of his right foot for 3 months causing functional disturbance. He was a heavy smoker and a bus driver by profession. There was no preceding history of trauma and no associated sensory or motor impairment of the foot. On examination there was a 5 x 3 cm pulsatile mass over the dorsum of the right foot without overlying skin changes (Figure 1A). The dorsalis pedis pulse was palpable immediately distal to the mass. The rest of his peripheral pulse examination was unremarkable. A duplex ultrasound scan demonstrated a true right DPA aneurysm (Figure 1B), confirmed by a subsequent computed tomographic angiogram (Figure 1C) with dimensions 40.5 x 25.6 mm. Other investigations, which included a complete blood count, C-reactive protein level, erythrocyte sedimentation rate and a 2D echocardiogram, were unremarkable.
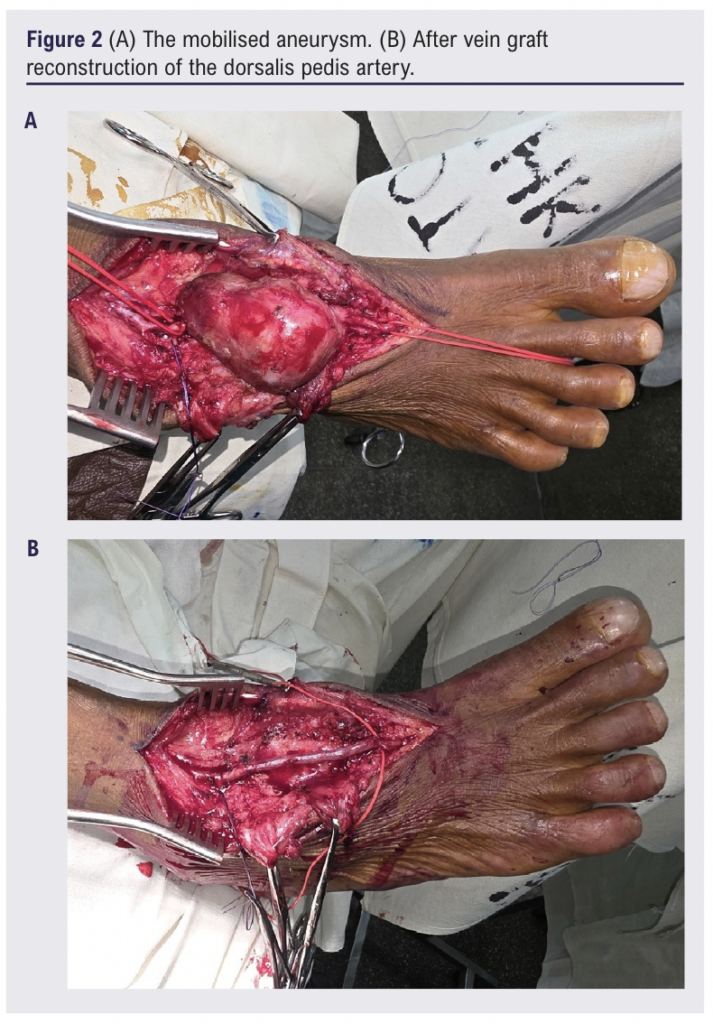
Under spinal anaesthesia, surgical repair of the right DPA aneurysm was undertaken. After proximal and distal control of the DPA, the mass was completely mobilised (Figure 2A) and the ipsilateral thigh GSV was harvested. Following systemic heparinisation and clamping of the DPA, the aneurysm was excised. The vessel was reconstructed using a reversed GSV graft (Figure 2B), with anastomoses using 7/0 polypropylene interrupted sutures.
Bacteriological culture of aneurysm tissue samples was negative. The patient’s postoperative recovery was uneventful apart from a minor superficial wound breakdown. Six months after surgery he remains well with a patent graft.
Discussion
True DPA aneurysms are rare, with the first case documented by Archibald Cuff in 1907.6 The majority of reported DPA aneurysms are false aneurysms related to trauma.2-4 True aneurysms, which are much rarer, have been associated with atherosclerosis, hypertension, smoking and minor repetitive trauma.2,3,7,8
The majority of DPA aneurysms present as a progressively enlarging pulsatile mass.2 Pain can result from pressure on the adjacent nerves.8 Functional impairment from the mass on the dorsal foot often prompts medical attention and subsequent intervention.9 This was also the case in our patient. Rarely, patients with these lesions can present with ischaemic complications due to thrombosis or embolism.5 Rupture is extremely uncommon.10
The diagnosis of DPA aneurysms involves clinical examination, supplemented by imaging studies. Duplex ultrasound is the preferred initial imaging modality. Angiography, whether non-invasive or invasive, offers additional details such as the presence of synchronous aneurysms and the adequacy of collateral circulation.1,4,10
Intervention is generally recommended for true DPA aneurysms. Due to the rare nature of these lesions, no size cut-off for intervention has been established but conservative management with follow-up may be an option for asymptomatic small aneurysms.3,8 Proponents of intervention, regardless of size or absence of symptoms, argue that early intervention can prevent future complications.1 Surgical resection of the aneurysm, with or without vascular reconstruction, can be performed with minimal morbidity. Ligation of the DPA without restoring vascular continuity should only be done after confirming adequate collateral circulation. Preoperative digital subtraction angiography to verify the patency of the foot arch, intraoperative Doppler assessment of the digital arteries after clamping the DPA and good back bleeding from the distal end of the DPA are indicators of good collaterals.2,4,8,10 Comparing the distal DPA stump pressure with radial artery pressure is another method used by Kato and colleagues to confirm sufficient foot perfusion after DPA ligation.11 For patients with risk factors for occlusive arterial disease such as diabetes and smoking and in children, where a ligated foot artery could affect growth, reconstruction is preferred.8,10 Options for reconstruction include end-to-end repair, vein patch repair or interposition grafting.8 Anastomosis with interrupted sutures may reduce the risk of luminal compromise in small vessels
Conclusion
True aneurysms of the DPA are rare and primarily dealt with by open surgery. Excision of the aneurysm and reconstruction of the artery is the preferred technique. Ligation of the DPA can be performed in selected patients who have robust evidence of adequate collateral circulation.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2026;5(3):156-158
Publication date:
May 27, 2026
Author Affiliations:
Department of Vascular Surgery, Teaching Hospital Kurunegala, Kurunegala, Sri Lanka
Corresponding author:
Thilina Gunawardena
Consultant Vascular and
Transplant Surgeon,
Department of Vascular Surgery, Teaching Hospital Kurunegala, Kurunegala, Sri Lanka
Email: [email protected]


")

")

