CASE REPORT
New onset arteriovenous malformations in adults: a case series of caution
Harker JJ,1 Godfrey D,1 Nickinson A,1 Baker T2
Abstract
Introduction: New onset arteriovenous malformation (AVM) in adulthood requires a high index of clinical suspicion. The misdiagnosis of vascular soft tissue lesions as AVMs is relatively common, resulting in delays to definitive diagnosis and management. We present four recent ‘AVM referrals’ which were neoplastic and propose some clinical considerations to facilitate development of a care pathway for AVM referrals.
Case reports: Four patients over a 6-month period were referred with ‘an AVM’ following clinical and ultrasound assessment. Ultimately these lesions were diagnosed to be neoplastic, including a Merkel cell carcinoma, an atypical fibroxanthoma with sarcomatous features, and two cases of relapsed marginal zone lymphoma.
Discussion: These cases demonstrate a range of features which are atypical for AVM. Atypical clinical features include sudden onset, rapid growth, pain or haematological malignancy in earlier life. Atypical ultrasound findings include failure to identify clear feeding vessels or a central nidus, and simple reporting of lesion vascularity. There is significant variation in ultrasound practices for vascular soft tissue lesions which do not follow a standardised protocol. Clinical decision making may be facilitated by complementary imaging and histological tissue sampling.
Conclusion: New onset AVM in adulthood with atypical clinical and ultrasound features should raise suspicion for malignancy. Such vascular soft tissue lesions require urgent investigation within a multidisciplinary setting to avoid delays in diagnosis and treatment.
Introduction
Arteriovenous malformations (AVMs) are rare vascular anomalies characterised by shunting of arterial blood into the venous system without an intervening capillary bed, leading to a high-flow pressure system. These malformations can manifest in various tissues and organs, presenting with a wide spectrum of clinical signs including pulsation, thrills, bruits and elevated local temperature.1,2 A wide range of malignant soft tissue tumours mimic AVMs due to associated neovascularisation or vascular invasion on ultrasound, leading to inappropriate referral and management plans with 40% of soft tissue sarcomas being misdiagnosed.3 This series outlines four recent referrals for suspected AVM in whom histopathological examination confirmed malignancy. These cases emphasise the need for clinicians to consider a broader differential diagnosis when encountering atypical vascular-appearing lesions labelled as AVM. All cases presented were fully counselled, consented and, in liaison with the appropriate multidisciplinary team (MDT), the lesions were excised (or biopsied) and sent for histological assessment. All cases have provided consent for use of their history and images for learning purposes.
Case reports
Case 1
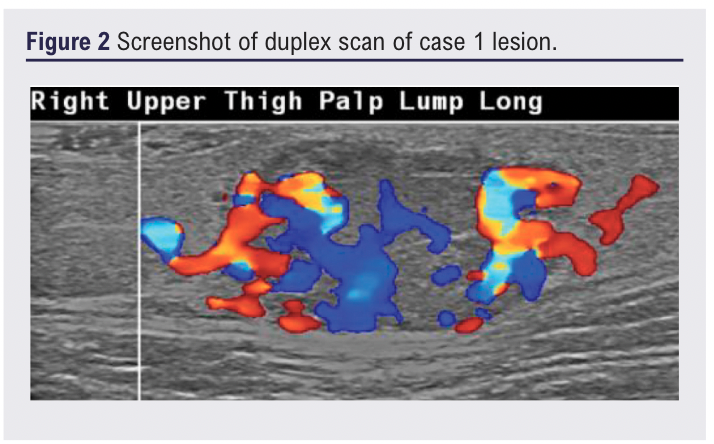
A 54-year-old man presented with an 18-month history of an enlarging painful lesion on the lateral right thigh (Figure 1). There were no systemic symptoms or lymphadenopathy. Handheld doppler examination identified an arterial signal adjacent to the lesion. Ultrasound was reported as a well circumscribed, hypoechoic, solid homogenous, hypervascular soft tissue lesion with arterial and venous flow seen (Figure 2). Subsequent CT indicated an arterial supply (profunda branch) without evidence of invasion or other abnormality identified, which was summarised as likely to be an AVM.
He was subsequently referred to the vascular service where excision biopsy was undertaken. Histology revealed a lobulated necrotising high-grade Merkel cell carcinoma with close peripheral and deep margins, staged as T2M0N0. He is receiving radiotherapy following marginal excision to the original lesion site.

Case 2
A 35-year-old man presented with a 12-month history of an enlarging blue-tinged nodule on the upper limb, reporting bleeding on contact, but without systemic symptoms (Figure 3). Ultrasound demonstrated an 18×14×15 mm well-defined hypoechoic lesion within the subcutaneous fat, with moderate arterial flow and suspected feeder vessels, reported as having features suggestive of a haemangioma or AVM (Figure 4). Referral to the community dermatology service was redirected to general surgery who, having reviewed the ultrasound report, redirected him to vascular services as a probable AVM.

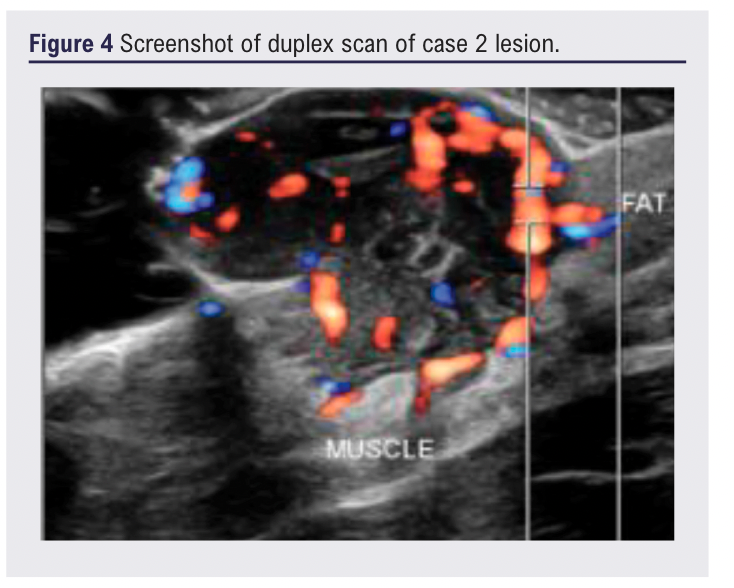
Given diagnostic concern, excision biopsy was undertaken with margins. Histology reported an excoriated atypical spindle cell tumour infiltrating into the subcutaneous tissue, showing high mitotic activity. Immunohistochemistry was negative for melanoma, epithelial and vascular markers but positive for CD10, suggestive of atypical fibroxanthoma but, due to deep infiltrative growth, significant atypia and location, a diagnosis of dermal sarcoma was favoured. At follow-up, a new skin lesion with similar clinical features has been identified on the lower limb which is pending further excision biopsy in addition to cross-sectional imaging for staging and decision on further management.
Case 3
A 75-year-old man with a history of B-cell lymphoma and prior splenectomy (for immune thrombocytopenic purpura) was referred with an enlarging posterior right thigh lesion. Ultrasound showed a 44×16×24 mm ill-defined heterogeneous lesion with serpiginous internal anechoic areas and marked vascularity (Figure 5).
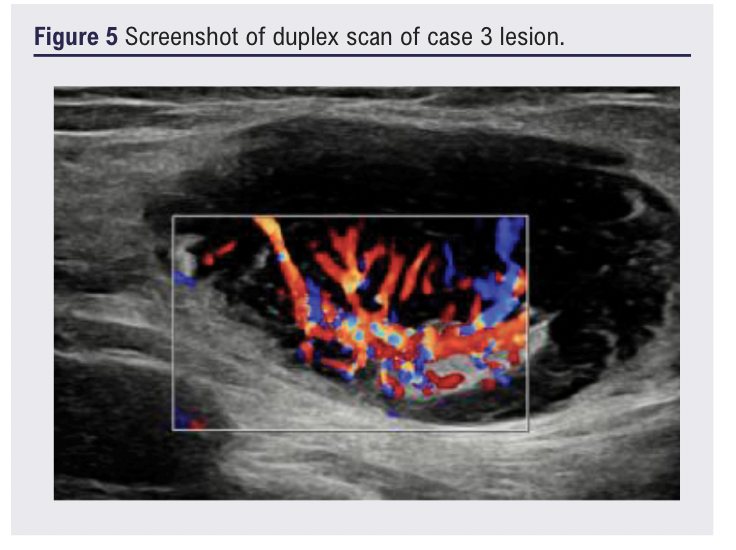
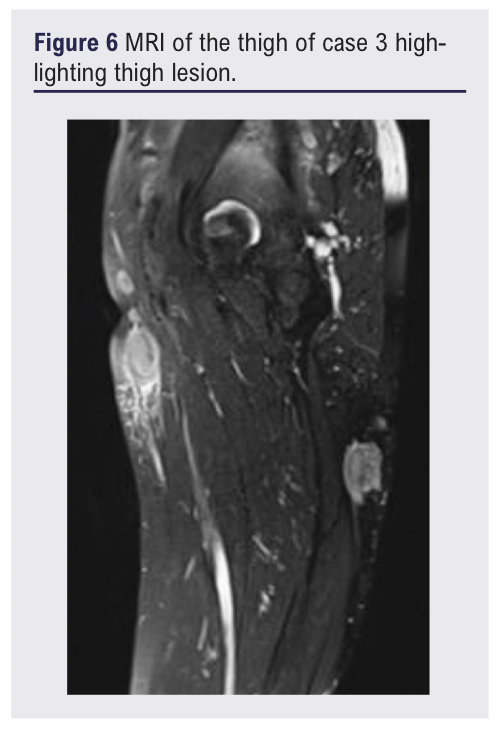
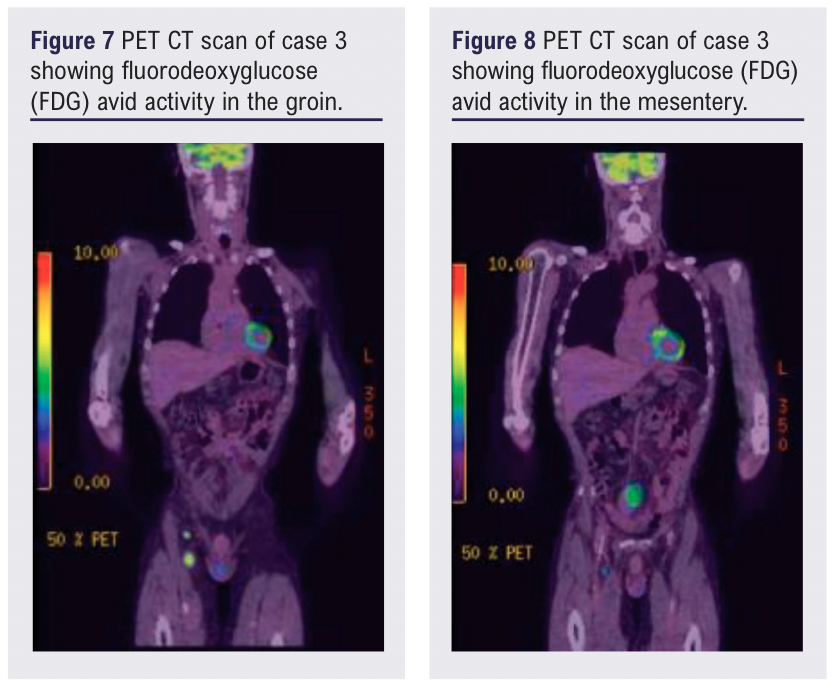
At review, a further lesion was clinically identified in the medial thigh corresponding to a 17 mm irregular hypervascular lymph node. Subsequent MRI (Figure 6) and CT positron emission tomographic (PET) imaging revealed a 44 mm mesenteric mass in addition to clinically identified lower limb lymph nodes with fluoro-deoxyglucose (FDG) avid activity (Figures 7 & 8).
Core biopsy showed complete architectural effacement and diffuse proliferation of small to medium-sized CD20+ and CD79a+ B-lymphocytes with a low Ki-67 proliferation index, consistent with low-grade B-cell lymphoma, favouring nodal involvement by marginal zone lymphoma. Treatment with chlorambucil and rituximab was initiated by the MDT and achieved a stable response.
Case 4
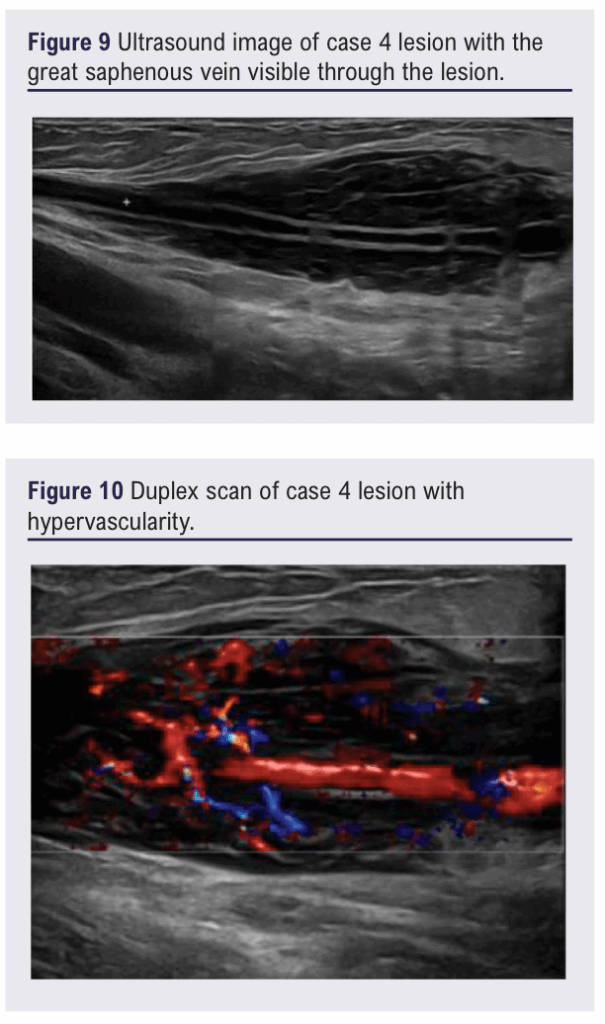
A 76-year-old man with a past history of extranodal marginal zone B-cell lymphoma treated with radiotherapy in 2016 presented with an enlarging left groin mass. Ultrasound showed a 90×22×41 mm fusiform hypoechoic cuff centred around the great saphenous vein. The lesion was reported as being hypervascular but was not affecting flow through the vein (see Figures 9 and 10). The sonographer felt an AVM was possible, prompting forward referral.
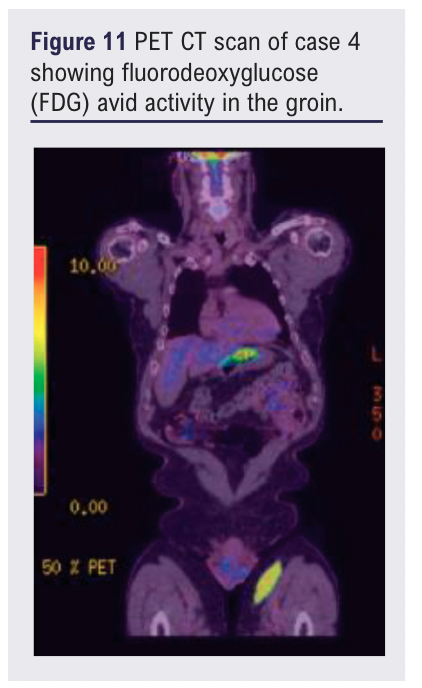
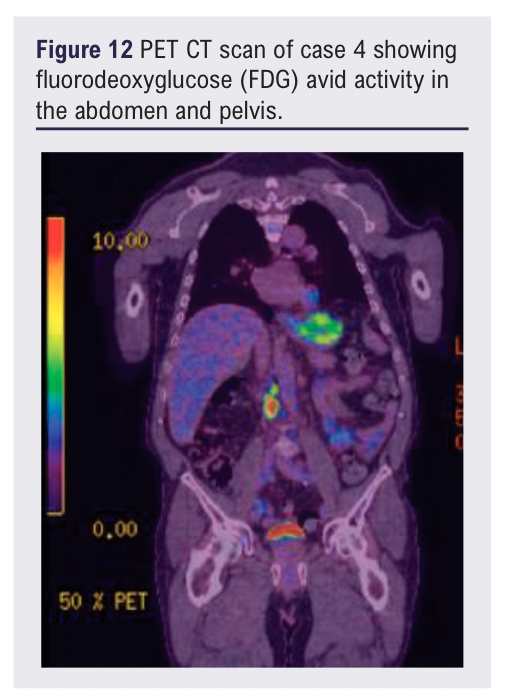
At review, in addition to the left groin mass, two lateral thigh lesions were identified. The patient was otherwise clinically well with no systemic symptoms. Subsequent MRI confirmed an 11 cm subcutaneous mass encasing the great saphenous vein without muscular invasion. A PET-CT scan showed FDG avid activity in the thigh lesions as well as the abdomen and pelvis (see Figures 11 and 12).
Core biopsy of the thigh lesion showed architectural effacement of lymphoid tissue, suspicious for marginal zone lymphoma recurrence. He was commenced on cycles of rituximab/ cyclophosphamide/ vincristine/ prednisolone (RCVP) for disease control.
Discussion
This contemporary case series demonstrates the pitfall of new onset ‘AVM referrals’ when originating from areas of limited clinical experience and reliance on non-protocolised ultrasound reports.
Epidemiological context is important in considering a diagnosis of AVM as most cases present early in life, and new true vascular lesions in adults are more likely to be acquired. Population-based studies suggest the prevalence of true AVMs in adults remains low, reinforcing the need to maintain a broader differential diagnosis in older patients presenting with vascular-appearing soft tissue lesions.4 Symptoms suggestive of alternative diagnoses to AVM commonly include – but are not limited to – sudden onset (without trauma or intervention), rapid growth ± regression period, bleeding and/or painful at rest and a past history of haematological malignancy.
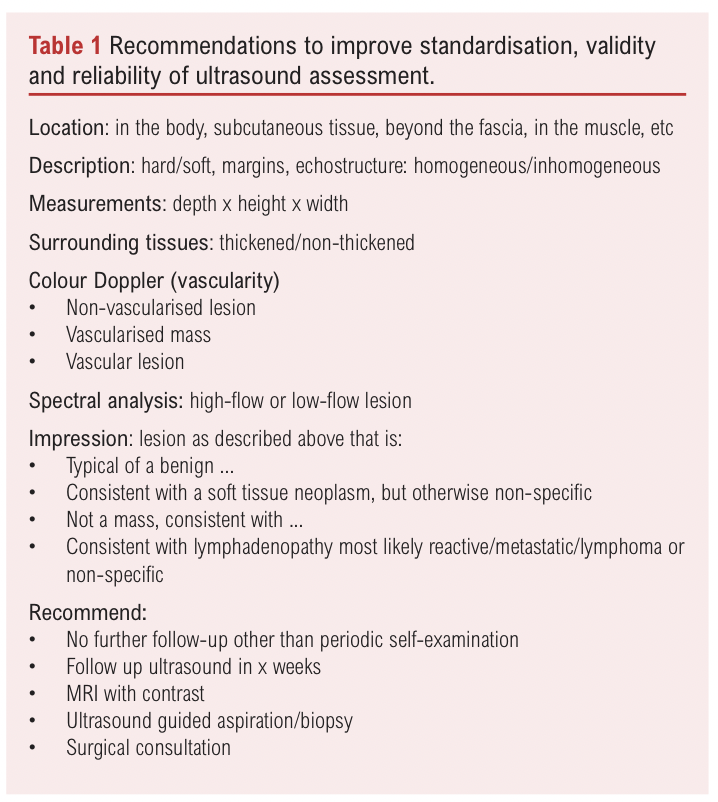
Due to ease of access, patients referred to secondary care services with a possible AVM have not infrequently undergone ultrasound assessment. However, possibly due to lack of guidelines, ultrasound assessment and reporting is variable. Soft tissue tumours are well known to exhibit increased internal vascularity due to angiogenesis or direct vascular invasion, resulting in ultrasound findings that can mimic AVMs.3,5,6 This overlap is well-documented, with malignancies including sarcomas and lymphoma being commonly mistaken for benign vascular anomalies.3,7 Recommendations to improve standardisation, validity and reliability of ultrasound assessment have been recommended (see Table 1).8,9
Where imaging is unclear or a high clinical suspicion exists for malignancy, tissue biopsy is critical in an MDT setting.6,7 Delays in obtaining tissue diagnosis, often due to perceived vascularity or fear of bleeding, can delay timely oncological diagnosis and treatment. Therefore, efficient MDT working across a range of specialities is important in complex or indeterminate cases and permits flexible approaches to ensure responsiveness and holistic care.
The role of advanced imaging modalities such as MRI and PET-CT is increasingly important when lesions exhibit atypical characteristics. PET imaging is particularly valuable in the assessment of marginal zone lymphoma and has been shown to correlate with disease burden and staging, especially in relapsed or extranodal presentations.10,11 This should be considered early in patient pathways where there is a history of adulthood haematological malignancy.
Classification of true vascular anomalies should be guided by international recommendations into vascular tumours (benign, borderline and malignant) and vascular malformations (fast or slow flow), which provide valuable information and inform decisions regarding further imaging and treatment.12,13
Conclusion
A thorough history and clinical examination remain the critical first step of ‘possible AVM’ assessment, supported by protocolised ultrasound examination and reporting. Atypical features should raise suspicions of underlying malignancies. In such cases, clinicians should have a low threshold for histological evaluation with complementary cross-sectional imaging, as part of a robust MDT, in order to reduce misdiagnosis and treatment delay.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2026;5(2):98-102
Publication date:
January 22, 2026
Author Affiliations:
1. Vascular Department, University Hospital Dorset, Bournemouth, UK
2. Vascular Department, University Hospital Southampton, UK
Corresponding author:
Mr Dean Godfrey
Vascular Consultant, University Hospital Dorset, Castle Ln E, Bournemouth BH7 7DW, UK
Email: [email protected]


")

")

