REVIEW
Psychological needs of individuals with peripheral arterial disease: a narrative review
Jubouri M,1 Hayden E,2 Kocsis A,2 Shalhoub J1
Plain English Summary
Why we undertook the work: Peripheral arterial disease (PAD) is a condition affecting blood flow to the legs, causing pain, reduced mobility, and, in severe cases, the risk of amputation. While physical symptoms are well understood, the impact of PAD on mental health, such as stress, anxiety, and depression, is often overlooked. This study reviewed existing research to better understand how PAD and mental health interact to influence with each other and to explore how psychological care could improve outcomes for these patients.
What we did: We reviewed studies from multiple scientific databases, focusing on the interaction between PAD and mental health. We also reviewed psychological assessment tools and therapies, including counselling and mindfulness, to see how they can help patients with PAD. For this, we conducted a thorough literature search using multiple search terms and electronic database.
What we found: Key themes included the role of life experiences, such as childhood trauma, and the benefits of mental health care integrated with physical treatment. Patients with PAD often experience depression, anxiety, and stress, which worsen their quality of life and ability to manage the disease. Life challenges, such as financial difficulties or traumatic childhood experiences, increase the likelihood of psychological issues in patients with PAD. Integrating mental health care with physical treatments like exercise therapy can improve both physical recovery and mental well-being.
What this means: Addressing mental health is vital for improving care for patients with PAD. Tailored psychological therapies, delivered as part of a multi-disciplinary team, can reduce distress, improve physical health, and enhance overall quality of life. Future research should focus on long-term benefits of such integrated approaches and explore better ways to identify and support patients with the greatest mental health needs.
Abstract
Background: Peripheral arterial disease (PAD) is a chronic, atherosclerotic condition that affects over 200 million individuals worldwide, with significant morbidity and mortality. While its physical manifestations, such as intermittent claudication and chronic limb-threatening ischemia, are well-established, the psychological burden of PAD remains underexplored. This narrative review aims to explore the psychological needs of individuals with peripheral arterial disease (PAD), highlighting the bi-directional relationship between PAD and mental health concerns.
Methods: A comprehensive literature search was conducted using strict search terms and multiple electronic databases including PubMed, Ovid/Medline, Google Scholar and Scopus. A systematic literature search identified key psychological themes, including the role of adverse childhood experiences (ACEs) in shaping mental health vulnerabilities and disease outcomes.
Results: The evidence underscores the bi-directional relationship between PAD and psychological concerns, as well as the urgent need for a multidisciplinary approach in PAD care. Integrating mental health professionals into vascular teams enables the provision of tailored psychological therapies, such as cognitive-behavioural therapy, mindfulness, and trauma-informed care. These interventions have demonstrated efficacy in reducing psychological distress, improving treatment adherence, and enhancing physical outcomes. Moreover, early identification of mental health concerns, especially in patients with high ACE scores or severe PAD symptoms, can guide individualised care plans to optimise outcomes.
Conclusion: Future research should explore the long-term benefits of integrated care models, addressing both physical and psychological needs. By prioritising mental health alongside traditional vascular interventions, clinicians can improve not only survival rates but also the holistic well-being of patients with PAD.
Introduction
Peripheral arterial disease (PAD) is an atherosclerotic occlusive process that involves the arteries of the extremities and burdens up to a quarter of a billion individuals globally. It is ranked as the third leading cause of atherosclerotic morbidity after coronary artery disease and stroke, making it one of the leading causes of disability. The incidence of PAD is known to increase with age, with nearly one in five of those aged over 60 being affected. Given the ageing population, both the incidence and prevalence of PAD will continue to rise.1 Diagnosis and severity of PAD are based on history, physical examination, walking distance, ankle-brachial pressure index (ABPI) assessment and arterial imaging. The hallmark presenting symptom of PAD is intermittent claudication, described as leg pain which occurs while walking. Other reported symptoms include altered peripheral sensation, cold extremities, muscle weakness and sexual dysfunction. These symptoms impair the mobility and functional ability of patients, leading to loss of independence, social deprivation, increased risk of other cardiovascular pathologies, reduced health-related quality of life (HRQoL)2,3 and disease progression. PAD is a pathological continuum that can progress to chronic limb-threatening ischaemia (CLTI) affecting nearly 6.5 million individuals globally, characterised by rest pain, non-healing ulcers or tissue loss which, if untreated, can result in limb amputation in about 30% of cases or even mortality in 25%.4 Not only is PAD a health burden to patients, but it is also a financial burden to health systems, with studies reporting annual costs reaching US$6.31 billion.5 The National Health Service (NHS)’s expenditure on treating PAD is a significant amount, with some studies estimating costs ranging from £4 million to over £206 million annually, depending on the specific treatments and populations involved.6
The mental health status of patients with PAD is also an important consideration. The psychological aspects of PAD are often overlooked or forgotten, particularly given the physical, social, financial and quality of life (QoL) burdens posed. The impact of PAD on mental health is being increasingly acknowledged, rising simultaneously with the growing incidence of PAD, as well as the increased adoption of the ‘bio-psycho-social’ model in modern practice, especially given the clinical relevance of mental health to all disease processes.7 Yet, while the physical manifestations of PAD are well established, the literature covering psychological manifestations remains limited. However, available evidence shows that the commonly reported mental health concerns secondary to PAD include stress, anxiety and depression. These, in turn, have been shown to be independently associated with functional impairment, as well as being known risk factors for suboptimal postoperative recovery.8,9
Beyond the psychological burden affecting many patients with PAD there is now evidence that a patient’s psychological history, particularly in the form of adverse childhood experiences (ACEs), impacts not only their risk of developing physical disease, including vascular disease, but can also impair their ability to interact with healthcare and to manage their condition. This has been shown to have a longitudinal negative effect, lasting well into adulthood.10 Hence, it is of interest and importance to explore the relationship between ACE and PAD.
This narrative review aims to explore the psychological needs of individuals with PAD, highlighting the bi-directional relationship between PAD and mental health concerns. The review also describes the current evidence on mental health impacts, ACE and psychosocial interventions, while identifying gaps in integrated care pathways.
Methods
We conducted a narrative review following the SANRA (Scale for the Assessment of Narrative Review Articles) guidelines.11 Searches were conducted in PubMed, Ovid/Medline, Scopus, and Google Scholar using Boolean combinations of terms including “peripheral arterial disease”, “PAD”, “mental health”, “depression”, “anxiety”, “stress”, “quality of life”, “psychological intervention”, “ACE”, “psychosocial”, and “multidisciplinary care”. We included English language articles from January 2000 to January 2024, focusing on studies of adults with PAD that reported psychological outcomes or interventions. Systematic reviews, observational studies, clinical trials and high-quality narrative reviews were included. Critical appraisal was conducted informally based on study design, sample size, use of validated assessment tools and relevance to PAD. Themes were inductively identified from recurring findings across studies.
Themes identified include QoL/HRQoL, disease acceptance and coping, patient activation, psychological therapies, ACEs and the incidence of psychological concerns such as anxiety, stress and depression (Table 1) as well as the impact of these on both physical/social functioning and clinical outcomes.

Overall, the body of literature exploring psychological aspects of PAD is heterogeneous in methodology and variable in quality. Most included studies were cross-sectional or observational in design, with a few systematic reviews and one non-randomised trial. While many studies utilised validated patient-related outcome measures (PROMs) and psychological tools, the absence of longitudinal designs limits causal inference. Several studies lacked adequate control for confounding variables, and reporting on recruitment procedures and attrition rates was inconsistent. Using informal criteria from the Newcastle-Ottawa Scale and ROBINS-I for non-randomised studies, methodological quality was generally moderate, with a moderate risk of bias in over half of the studies due to self-reported outcomes and lack of blinding. This underscores the need for robust, longitudinal and interventional research designs.
Measurement tools
Several tools have been developed globally to assess the mental and social health of patients, as well as their HRQoL. These tools are often known as PROMs. These questionnaires can be used either generically to assess patients’ overall health or as disease-specific tools focused on PAD. It is important to note that disease-specific PROMs exhibit higher sensitivity and specificity relative to generic ones.12 Another way of categorising PROMs includes those tools which cover the full spectrum of PAD, or other tools which can be applied to subtypes on that spectrum. In the case of PAD, disease-specific PROMs include the peripheral artery disease quality of life questionnaire (PADQOL), vascular quality of life questionnaire (VascuQoL), Australian vascular quality of life index (AUSVIQUOL), peripheral artery questionnaire (PAQ), intermittent claudication questionnaire (ICQ), walking impairment questionnaire (WIQ) and Edinburgh Claudication Questionnaire. Meanwhile, key examples of generic PROMs are the EuroQoL-5D (EQ-5D-3L), Nottingham health profile (NHP), 36-item short form (SF-36®), McMaster Health Index and World Health Organization Quality of Life Assessement-100 (WHOQOL-100) tools.4,12,13 However, the validity and full applicability of these PROMs remain an area for further investigation.14 A summary of these PROMs can be found in Table 2. With regard to psychological assessment, commonly used questionnaires include the Generalized Anxiety Disorder-7 (GAD-7) and the Patient Health Questionnaire-9 (PHQ-9).4,12,13

A 2018 systematic review identified themes from qualitative research related to PAD patients’ HRQoL using a framework analysis.4 The qualitative framework analysis was divided into six main groups: symptoms, impact on physical functioning, impact on social functioning, psychological impact, financial impact and process of care. When results of this qualitative analysis were mapped against the items/domains contained in 43 validated PROMs used in patients with PAD, the results revealed that neither the generic nor disease-specific PROMs cover the full spectrum of PAD or disease domains. However, the authors concluded that NHP and VascuQoL can be considered the optimal generic and disease-specific PROM, respectively.4 Nevertheless, these findings indicate a possible gap in both clinical and research practices whereby solely relying on PROMs to wholly capture the experience of patients with PAD may be misaligned with patients’ true needs.
Influence of PAD on mental health
The evidence linking PAD and mental health is limited within the current literature, which can be partly attributed to the lack of clinical infrastructure combining both physical and mental health in the holistic management of individuals with PAD, particularly in light of the aforementioned deficit in the screening tools used. The majority of evidence on this topic stems from cross-sectional studies using one or a combination of the above tools to measure HRQoL, disease burden and acceptance, depression, stress and anxiety and patient experience.15-27 The studies which looked at PROMs do not, in the main, take ACE into account, and are cross-sectional. This means that we have little evidence on causal relationships. Furthermore, we do not have detailed data which could guide the stratification of patients in terms of the likelihood of needing support nor the effectiveness of different approaches to the delivery of their healthcare.
A cross-sectional path analysis was recently conducted on a cohort of 1696 patients with PAD using a theory-based model.1 The mean age of the cohort was 66.29±8.63 years and 67.6% (n=1141) were male. Risky alcohol consumption, defined by an AUDIT-C score of >4 in females and >5 in males, was reported by 29.1% of participants. Using the Fagerström test for nicotine dependence, 26.9% and 16.8% were identified as having either strong (5–6) or very strong (7–10) dependence on tobacco, respectively. That being said, it is important to note that the study used path analysis to account for potential confounding factors, including sociodemographic characteristics and baseline co-morbidities, which yielded a better fit between the goodness-of-fit indices and the observed data. The main analysis identified that walking difficulties due to PAD were linked to higher levels of depressive (β=−0.36, p<0.001) and anxiety symptoms (β=−0.24, p<0.001). Moreover, it was estimated that 5.5% and 2.7% of the patients experienced severe depressive and anxiety symptoms based on the PHQ-9 and GAD-7 surveys, respectively. Overall, the prevalence of depressive and anxiety symptoms of any severity stood at 48.3% and 35.5%, respectively, with female and younger patients being more susceptible. Walking impairment negatively impacted the physical QoL both directly (β=0.60, p<0.001) and indirectly through depressive symptoms (β=−0.16, p<0.001); it also had an indirect adverse effect on mental QoL, mediated through depressive (β=−0.43, p<0.001) and anxiety symptoms (β=−0.35, p<0.001). The authors described the involvement of addictive behaviours in the psychological sequela by reporting a significant association between depressive symptoms and tobacco use in their cohort, which also interplays with PAD pathogenesis.1
The 2023 Scientific Statement released by the American Heart Association (AHA) tackled these issues in further depth.8 This statement was the result of an integrated PAD team collaboration involving both vascular surgeons and clinical psychologists along with other healthcare professionals. In addition to symptoms of depression, anxiety and stress, the statement also outlined the issue of addiction (opioids, alcohol, tobacco) secondary to PAD, giving examples of addictive opioid use in approximately 25% of the PAD population. The statement also acknowledged that addiction is more common in those also suffering from depression.
Furthermore, problematic substance use has been proven to be present in more than 60% of individuals with CLTI and is known to negatively influence revascularisation outcomes. The AHA also pointed out a correlation between increased risk of PAD and other mental health disorders such as post-traumatic stress disorder and attention-deficit/hyperactivity disorders. Other relevant manifestations of PAD include cognitive impairment and sleep disturbances. Lastly, the authors recognised the association of ACE with higher risks for cardiovascular diseases and premature mortality, and recommended the integration of ACE assessment into the holistic management of PAD.8
In a multicentre international prospective study of 1275 patients with PAD, 957 (75.1%) completed screening for mental health concerns on initial presentation to vascular clinics.15 Three hundred and thirty-six patients (35%) exhibited symptoms of depression, anxiety or perceived stress, of which 73 (7.6%) had two concerns and 40 (4.2%) showed all three. The Patient Health Questionnaire-8 (PHQ-8), Generalized Anxiety Disorder scale-2 (GAD-2) and Perceived Stress Scale-4 (PSS-4) were used to assess mental health concerns, and showed that stress was most commonly reported (28.7%), followed by symptoms of depression (14.1%) and anxiety (8.3%). Those exhibiting any psychological symptoms were more likely to be female, younger, of lower socioeconomic status, with less health and social support.15 Clinically, these patients were also more likely to have suffered from co-morbid neurological events, diabetes, coronary heart disease and previous depression. Nevertheless, a significant reduction in the above concerns was observed at the 12-month survey, with reported rates of stress, depressive symptoms and anxiety dropping to 17.5% (p<0.001), 8.9% (p=0.02) and 5.7% (p<0.001), respectively. Despite this, the authors identified that a considerable percentage of patients screened positive for psychological symptoms for the first time at the 12-month follow-up: 42.3% for depression, 67.3% for anxiety and 46.7% for perceived stress. These individuals, who showed new psychological symptoms one year after coming into the study, but not at enrolment, were more likely to have had a previous history of depression.15 This is important because it is rare evidence of a potential causal role of the PAD diagnosis in exacerbating psychological symptoms, especially in individuals who are vulnerable to depression and anxiety at clinical levels. This was a robust study and is further evidence for the inextricability of life experience and the importance of recognising that, especially amongst those with difficult life histories and current circumstances, their psychological well-being needs to be addressed alongside medical interventions.
A systematic review of 28 studies which focused on the incidence of depression associated with PAD reported a prevalence of depression or depressive symptoms ranging from 11% to 48% in 12 cross-sectional studies and from 3% to 36% in 16 longitudinal studies.16 Fifteen different scales and tools were used to assess for depression in the included studies including the Beck Depression Inventory (BDI), Cambridge Mental Disorders of the Elderly Examination (CAMDEX), Center for Epidemiologic Studies-Depression Scale (CES-D), Geriatric Depression Scale (Short-form or 15-item versions) (GDS), General Health Questionnaire-12 items (GHQ-12), General Health Survey (GHS), German National Health Interview and Examination Survey–Mental Health Supplement (GHS-MHS), Hospital Anxiety and Depression Scale-14 items (HADS-14), Hamilton Rating Scale for Depression-17 items (HAM-D-17), Munich-Composite International Diagnostic Interview (M-CIDI), Patient Health Questionnaire (PHQ; 9-item or 12-item versions), Dutch-Present State Examination (Dutch-PSE), Zung Self-Rated Depression Scale (ZSRDS) and ICD-9 codes related to depression.16 Depressed PAD patients were again more likely to be younger, female, African-American (compared with Caucasian) and to have more frequent and/or severe PAD symptoms and functional impairment than non-depressed patients. Most of the included studies met most, if not all, of the Newcastle-Ottawa Scale criteria for a methodologically rigorous study. However, nine of the scales solely relied on patient-reported measures of depression as the exclusive criteria for diagnosis without a clinician’s verification, of which only six are considered well-established in this population. Hence, the study stressed the importance of using sensitive screening tools capable of detecting atypical symptoms that can manifest in some populations such as the elderly, which represents an area for further research and development.16
Bidirectional relationship between mental health burden and PAD
It is important to note, however, that the relationship between PAD and mental health is, as far as can be ascertained, complex and dynamic. On the one hand, psychological issues can exacerbate both the likelihood of physical disease and the ease of symptom management and, on the other, the presence of physical difficulties can cause or exacerbate low mood and anxiety, especially in those who are already vulnerable due to life experience or circumstances. This interaction can, unless identified early through a collaborative multidisciplinary approach between vascular surgery and psychology teams, result in further harm to both the patient’s physical and mental health.17
Ragazzo et al18 studied 113 patients with intermittent claudication. Using the BDI and BAI tools, 40% of patients were found to suffer from mild or moderate depression and 26.2% from anxiety of any severity. Patients with signs of depression were identified to have a shorter pain-free walking distance (p=0.015) and shorter total walking distance (p=0.035) than controls without depression signs. Furthermore, patients with moderate to severe depression reported significantly more barriers to physical activity than those with anxiety (p<0.005). However, anxiety alone did not have a significant effect on outcomes (p>0.05), although a degree of data overlap was observed with some patients being both anxious and depressed.18 Of note in this study, though, was the exclusion of patients with a previous history of depression or anxiety, in that they had previously received medication for mood. As we saw previously, it is likely that those with a history of struggling with mood would be vulnerable to exacerbation when faced with a new physical difficulty.
Aquarius et al13 undertook a single-centre cross-sectional study of 188 PAD patients focusing on patient-reported health burden and QoL. A similar trend to the above was seen, in that perceived stress was a significant predictor of a reduction in maximum walking distance (p=0.001) and poorer QoL (p<0.001). Stress was also identified to have a significant impact on the overall health of individuals with PAD (p<0.001), emphasising the importance of the bio-psycho-social model in this clinical context. In this study, stress was measured using the short 10-item version of the Perceived Stress Scale, health status using the RAND 36-Item Health Survey (RAND-36) and QoL using WHOQOL-100.13
Jelani et al19 analysed sex discrepancies in a cohort of 1243 patients with a higher incidence of moderate/severe depression (21.1% vs 12.9%; p<0.001) as well as mean depression score (5.6+5.3 vs 4.2+4.8; p<0.001) measured using the PHQ‐8 in females with PAD. After stratification by sex and clinically relevant depressive symptoms (PHQ‐8 >10), mean PHQ‐8 scores among those with depressive symptoms were similar between men and women (14.2+3.7 vs 14.1+3.7). In this sex-adjusted model, both male and female patients with depressive symptoms were more likely to be younger and sedentary compared with their respective counterparts without depressive symptoms. Furthermore, there was a tendency to avoid care because of cost; however, this needs to be taken in the context that this study was set in health systems where private health insurance plays a significant role. Additionally, this analysis showed that those with depressive symptoms had worse health status at each follow-up point (all p<0.0001).19 Another systematic review followed a similar trend in its vascular outcomes, reporting a 20% increase in the incidence of major adverse limb events in depressed patients.20
Clinical outcomes
The results of a study by Chyrek-Tomaszewska et al21 shed light on the critical relationship between depression and PAD revascularisation outcomes, which is an area with limited data. The PAD revascularisation group (n=159) experienced more frequent symptoms of depression and anxiety compared with healthy control individuals (n=160), measured using the HADS. The two groups were similar at baseline in terms of gender (p=0.72). Importantly, these symptoms were found to be associated with the severity of PAD based on ABPI measurements. A significant positive correlation was demonstrated between anxiety, depression symptoms and the intensity of walking pain. Multivariate analysis revealed that only amputations significantly increased anxiety severity, whilst depressive symptoms were influenced by multiple factors including previous revascularisation and amputation procedures as well as the severity of pain upon admission to hospital. A higher rate of severe depression was observed in those who underwent open surgical revascularisation compared with endovascular (10.5% vs 2.5%; p=0.0003).21 Importantly, a recent meta-analysis of five observational studies including a total of 119,123 patients, of whom 16.2% had depression or depressive symptoms, reported a 24% increase in mortality in this population compared with counterparts with no documented history of mental health conditions.22 In two of the five studies, depression was defined by an ICD-9 diagnosis code for Major Depressive Disorder or an equivalent, whilst the remainder used validated self-report screening tools including the GHQ-13, HADS and GDS. Overall, a moderate risk of bias was found using the Risk of Bias in Non-randomized Studies-of Interventions (ROBINS-I) instrument.23
Welch et al24 presented the relationship between PAD and mental health from a different perspective. In their study from June to August 2022, 37% of 104 individuals with PAD had at least mild depression on the PHQ-9. Meanwhile, 18% of the cohort had a documented history of depression, of whom 26% did not have a current antidepressant prescription. Moreover, 57% of those with a prescription still had an elevated PHQ-9 score despite the initiation of pharmacological treatment. These findings indicate the possible under-diagnosis and under-treatment of patients with PAD whose disease state is causing, or is associated with, psychological distress, with men being more likely to have unrecognised depression.24 This should be a major healthcare concern. In their first assessment of 148 patients with PAD treated between July 2015 and October 2016, a similar trend of under-diagnosis had been seen, with 28.4% of patients screening positive for depression using GDS-SF, whereas the documented prevalence was only 3.3%. The authors also reported a significantly higher mortality rate within 6 months of revascularisation for depressed patients compared with counterparts with PAD but no documented history of mental health conditions (9.5% vs 0.9%). Interestingly, the baseline patient characteristics in both groups were similar. Conversely, despite the significant association between depression and 6-month all-cause mortality on multivariate analysis, this was not the case for vascular reintervention, readmission or length of stay.24
Patient activation and coping
A cross-sectional study of 212 patients closely explored disease acceptance and coping in vascular patients (n=104) and surgical patients (n=108).25 The authors used the Acceptance of Illness Scale (AIS), which comprises five categories for coping ranging from ‘very well’ to ‘very badly’ and three categories for acceptance being ‘low’, ‘average’ and ‘high’. Lower self-assessment scores for coping with disease were reported in the vascular group relative to surgical counterparts (very well: 13% vs 25%, p=0.088). Disease acceptance was also found to be significantly lower in vascular patients than in surgical patients (low: 34% vs 14%; average: 33% vs 36%; high: 32% vs 50%, p=0.000).25 Connected to this, a systematic review of 14 qualitative studies encompassing 360 patients highlighted first-hand accounts of patients’ experiences of living with PAD.26 A key finding was the lack of patient understanding of their condition, which resulted in both delayed diagnosis and impaired adaptation once a diagnosis was made, which compounded the negative impacts of PAD on their QoL in different dimensions.26 These studies showcase the importance of effective communication and patient education, as well as the direct impact they can have on the quality of care delivered and subsequent clinical outcomes.
A 2011 report using multivariate modelling showed that patient activation is directly and strongly connected to clinical outcomes.27 This forms a pivotal component of the PAD treatment strategy and is a measure of patients’ understanding, competence and willingness to take responsibility of their healthcare decisions. In the context of vascular surgery, Humphries et al28 demonstrated variable activation rates reported by their cohort depending on disease type, length of symptoms and patient demographics using the 13-item Patient Activation Measure (PAM-13) survey. However, the authors observed higher levels of patient activation measures in their PAD population relative to other vascular diseases such as carotid, aneurysmal and venous disease, with CLTI patients being particularly activated (24% Level 1 activation, 34% Level 2 activation, 31% Level 3 activation, 34% Level 4 activation).28 The evidence cited above demonstrates the role that mood plays in activation. Depression is associated with less walking, as is anxiety, perhaps due to fear of pain. Therefore, understanding the context, beliefs and cognitions of patients, as well as providing reward and encouragement for effort, especially for those with the most challenges, is an important aspect of medical management.
In relation to the early findings of the vulnerability conferred by pre-existing psychological conditions, it is important to consider the evidence on the earliest types of injury that can affect later disease presentation and progression – namely, ACE.29 Felitti’s group was the first to use a questionnaire to measure ACE and to identify the dose-response relationship between ACE and physical disease.30 Since then, many studies have explored how ACE can affect the risk of developing chronic health conditions. This effect of toxic stress is direct on the one hand (increasing cortisol levels and chronic low-grade inflammation, for example) and indirect on the other, via the behaviours adopted to mitigate the psychological consequences of ACE (eg, problematic use of alcohol and non-prescription drugs, smoking and lack of motivation to exercise and over-eating, which can lead to obesity).30 There is also evidence that these behaviours are themselves mediated by neurodevelopmental failure to thrive when such ACEs are present.31
In terms of predicting risk, Bertele et al32 found, in a thorough psychiatric and cardiac evaluation of 210 adults, that ACE predicted epicardial adipose tissue and that this effect was mediated by both depression and lack of physical activity. Sonu et al33 analysed data, stratified by age, from nearly 90,000 adults recorded in the 2011–2012 Behavioural Risk Factor Surveillance System (BRFSS). They found that young adults with high ACE scores are at an increased risk of early-onset chronic disease, including cardiovascular disease. The adjusted incidence rate ratio (IRR) for cardiovascular disease between those with a null ACE score and those with a score of 4 or more was highest in the 18–34-year age group (IRR 2.57 (1.44–4.60). The authors point out that earlier onset of risk factors for cardiovascular disease affects lifetime risk.33
What are the consequences of ACE then, not only on the incidence of PAD but on its management? Neglect, abuse and chronic stress in childhood are also known to affect relationships in later life and, as we have seen, limit behaviours linked to self-care. Martin-Higarza et al34 collected detailed data from a sample of 170 individuals and found lack of proactive coping, attachment difficulties and financial hardship in those with higher ACE scores. It is understandable, therefore, that patients with such vulnerabilities present to their clinicians as more anxious, more ambivalent about treatment and less proactive. Their relationship to help, given the attachment ambivalence, is also likely to make them either more needy of attention and reassurance or less reliable attenders, or indeed both.
Interventions
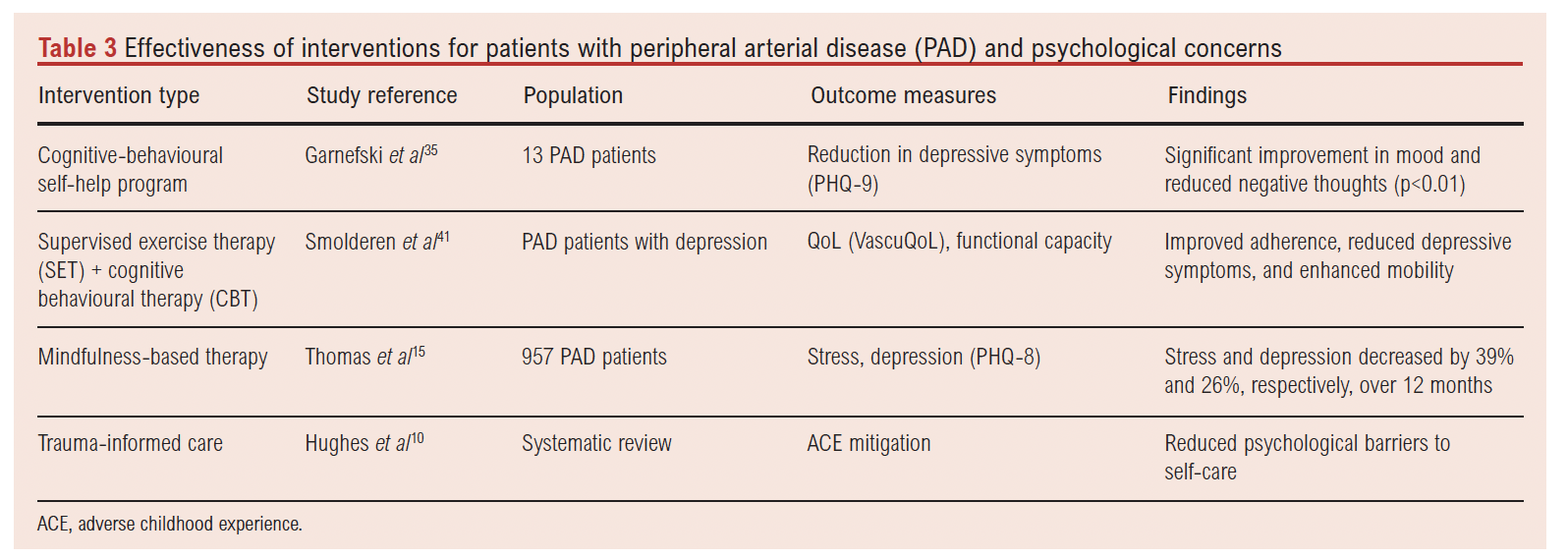
Evidence related to psychosocial inventions and their effect on PAD is very limited. A 2013 single-arm non-randomised clinical trial investigated the efficacy of a cognitive-behavioural self-help program.35 A total of 13 patients with PAD and mild to moderate depressive symptoms at baseline, determined by a PHQ-9 score of <5 and <14, were recruited from an outpatient vascular surgery clinic into the psychological programme. The intervention consisted of a workbook, a work programme and a computer-based programme with minimal coaching. The results of the pre-test, post-test and follow-up questionnaires showed a significant reduction in depressive symptoms, physical tension, negative thoughts and goal obstruction following the intervention (p<0.01).35 Despite its small sample size, this trial represents a solid foundation for future studies evaluating management strategies in this clinical scenario. In general, self-managed care interventions represented by lifestyle and behavioural changes such as smoking cessation, exercise engagement and healthy behaviours have been shown to have an overlapping positive impact on both PAD and mental health. Nevertheless, there is a lack of sufficient evidence supporting the role of dietary changes in this clinical context.4,35
Based on the above evidence, it is suggested here that pilot programs to evaluate standard of care should address the co-morbid psychological needs of individuals with PAD. These would include a structured pathway for early recognition of mood changes with appropriate escalation and referral pathways to specialists, streamlining the trajectory for optimising both PAD and psychological outcomes.8 Importantly, activating the full potential of any of the above measures requires the active involvement of patients in their own care. However, ACEs represent a potential obstacle to patient activation, with patients’ prior experiences influencing both their behaviours and how they engage in behaviour change. This is evident in several studies in the literature reporting significantly lower patient activation in patients with greater numbers of ACEs.36,37 Therefore, early identification of such individuals is likely to be of major importance so that more tailored and intensive approaches can be offered, taking into account the increased complexity and potential for re-traumatisation involved in such clinical scenarios.
Table 3 summarises available interventions aimed at improving psychological outcomes in PAD. Although evidence is sparse, cognitive-behavioural self-help programmes and supervised exercise therapy combined with cognitive behavioural therapy show promise. The study by Garnefski et al35, despite a small sample size (n=13), demonstrated statistically significant improvements in mood (p<0.01). However, larger randomised trials are needed to confirm efficacy. Mindfulness interventions, particularly when integrated into vascular care clinics, yielded sustained reductions in depressive symptoms. These findings support a stepped care model, where brief scalable interventions can be delivered early in care pathways.
Vascular surgery and psychology: How can we work together?
Addressing well-being in patients with PAD must involve a multidisciplinary approach that targets both mental and physical elements. Research highlights several strategies that vascular surgeons and psychologists can use to improve outcomes in an integrated care model.38 Vascular surgeons can lead the way to the optimisation of physical health in several ways other than revascularisation. For example, supervised exercise therapy, particularly walking programmes, have been shown to significantly improve functional capacity and quality of life.39 However, studies investigating the effectiveness of supervised versus unsupervised exercise therapy do not stratify patients in terms of mood. We would suggest that, by measuring mood, it would be possible to focus more attention and encouragement on those with the least motivation and the greatest fear of pain.
Smoking cessation is critical, as well as optimising medical therapy with antithrombotic agents, lipid-lowering and other medications to manage PAD symptoms and treat risk factors (eg, hypertension, diabetes), which improve vascular health and reduce symptoms, which can also have a positive effect on mental health.8,40 Additionally, patient education and empowerment play a major role, as does educating patients about PAD, its symptoms and the benefits of lifestyle modifications; encouraging active participation in treatment plans to increase adherence and to reduce feelings of helplessness as described in the above studies. While, traditionally, physical and mental health services offer separate interventions, there is opportunity for using psychological models such as motivational interviewing, behavioural economics, cognitive behavioural therapy and mindfulness-based interventions within the exercise programmes offered in the clinic.8,41 Such simultaneous and collaborative efforts from psychology teams could also help to reduce the stigma that some patients can feel if they are referred by their physician to psychology.42
Moreover, psychologists can promote health behavioural changes through techniques such as motivational interviewing and behavioural activation techniques, as well as addressing health beliefs and maladaptive thoughts that may hinder lifestyle changes.43 The aforementioned trial by Rezvani et al1 showed not only the significant correlation between PAD symptoms and depressive/anxiety symptoms, but also stressed that risky health behaviours should be approached by promoting behaviour change, which is typically delivered and/or supported by psychologists.1 These personalised care plans tailor interventions to individual patient needs – for instance, prioritising mental health interventions in patients with severe depression while focusing on physical rehabilitation for those with mobility issues.
Stratifying patients with PAD who have mental health concerns is essential to ensure that those most in need receive appropriate care. A collaborative approach between vascular surgery and psychology teams can enhance patient outcomes through routine implementation of mental health screening of patients with PAD using an appropriate combination of aforementioned PROMs in addition to functional status evaluation, both of which should be implemented periodically.8,15 This allows for timely adjustments to the care plan as needed. Furthermore, as seen in the above results, PAD patients who are female, younger, experiencing financial strain or lacking social support are at higher risk for mental health concerns, as are those with high ACE scores and a pre-morbid history of clinical depression and/or anxiety.1,15,16,19 Therefore, identifying these factors, summarised in Table 4, can help prioritise patients for comprehensive mental health evaluation alongside PAD management.15
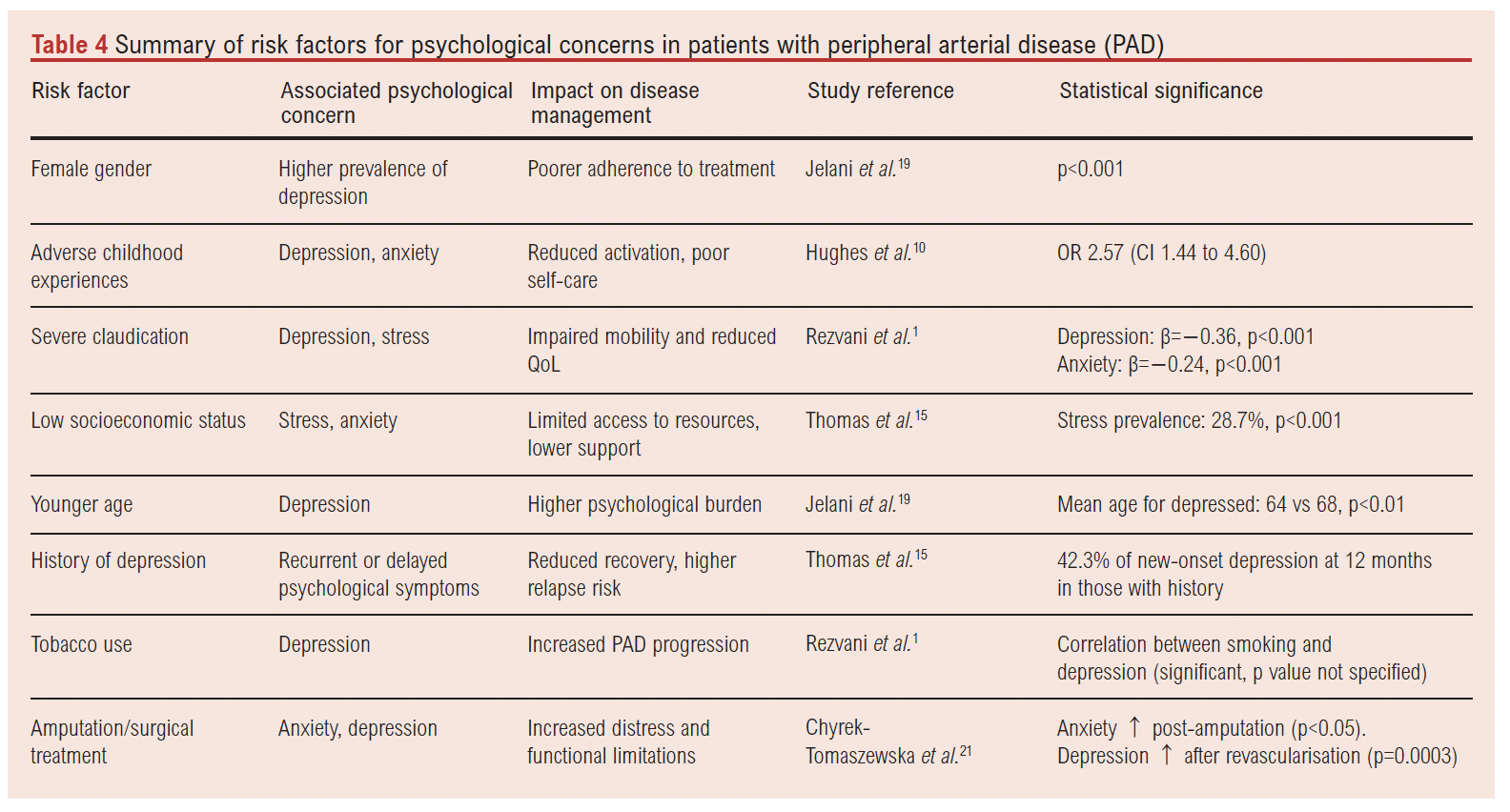
Table 5 provides a stratification framework for clinicians to tailor interventions based on patient risk profiles. High-risk individuals, such as those with severe PAD symptoms and high PHQ-9 scores, may benefit from more intensive interventions including cognitive behavioural therapy and trauma-informed care. In contrast, those with moderate or transient symptoms may be managed with education and mindfulness practices. This triaging approach ensures that mental health resources are allocated efficiently and that patients most in need receive timely psychological support.

Barriers to implementation within the NHS, including limited psychological service capacity, fragmented care pathways and stigma related to mental health, must be addressed to operationalise integrated care models for PAD.
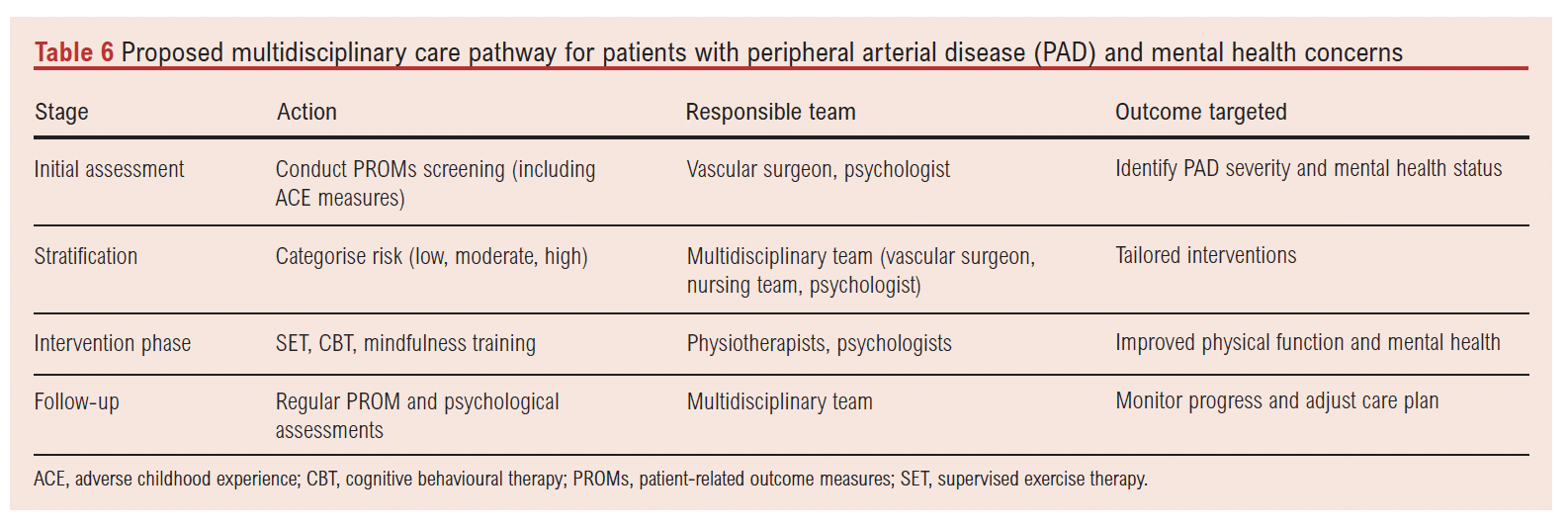
In summary, a multidisciplinary approach integrating vascular surgery and psychology is pivotal in managing PAD patients with mental health concerns. Vascular interventions, paired with psychological support, can improve adherence to treatments like supervised exercise therapy and smoking cessation, while cognitive behavioural therapy can mitigate depression and anxiety. This stratified strategy addresses the bidirectional relationship between physical and mental health, optimising outcomes as proposed in Table 6.
Conclusion
The mechanisms linking PAD pathogenesis and psychological status are clearly complex. On the one hand, existing mental health difficulties raise the probability of the occurrence of PAD and make it more difficult for people to activate changes necessary for mitigation. In other words, they continue with the behaviours that increased the likelihood of incidence.
There is also evidence that perceived stress (in particular) and concomitant anxiety and depression, even if new, can impact management. A person-centred approach, which takes the patient’s context into account, is likely to yield cost savings in the long run by delaying and potentially reversing PAD-related damage. Future research efforts should focus on strategies for early identification and management of psychological concerns in PAD to tackle both incidence and progression, constituting a pivotal step towards optimising outcomes in PAD. The implementation of structured specialist pathways, including clinical health psychology input, is crucial for improving the standard of care delivered to patients with PAD. Finally, study quality across the included literature was variable, with most studies being observational and cross-sectional in design, limiting causal inference. While many employed validated psychological and quality of life measures, inconsistencies in methodological rigour, sample sizes and control of confounding factors were common. These limitations highlight the need for higher quality, longitudinal and interventional research to better understand and address the psychological needs of individuals with PAD.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2025;4(4):169-180
Publication date:
August 19, 2025
Author Affiliations:
1. Section of Vascular Surgery, Department of Surgery and Cancer, Imperial College London, London, UK
2. Department of Clinical Health Psychology, St. Mary’s Hospital, Imperial College Healthcare NHS Trust, London UK
Corresponding author:
Joseph Shalhoub
Section of Vascular Surgery, Department of Surgery and Cancer, Imperial College London, London, W12 0NN, UK
Email: [email protected]


")

")

