CASE REPORT
Rare vascular complication of total hip arthroplasty: common femoral artery perforation diagnosed two months postoperatively
Mouhanni S, Mouyarden O, Farah S, El Jamaaoui A, El Bhali H, Azghari A
Abstract
Background: Vascular injuries complicating total hip arthroplasty (THA) are uncommon, with reported incidences between 0.2% and 0.42%. When they occur, they can threaten both the patient’s life and functional prognosis of the limb.
Case report: We describe a 38-year-old woman with tuberculous coxitis who underwent THA. Two months later she presented with acute back and groin pain associated with severe anaemia. Exploration revealed a perforation of the common femoral artery (CFA). Reconstruction using reversed saphenous vein bypass and profunda femoris reimplantation resulted in successful recovery.
Conclusion: CFA perforation after THA is exceedingly rare and may present late. Any unexplained groin symptoms or anaemia following THA should trigger urgent vascular evaluation.
Introduction
Arterial complications following total hip arthroplasty (THA) are rare but potentially devastating, with incidence estimated between 0.2% and 0.42%.1,2 Mechanisms include penetrating trauma from retractors or screws, traction injury during dislocation, perforation during acetabular preparation, or delayed vessel erosion leading to pseudoaneurysm formation.3 Revision surgery, dysplasia and pelvic fractures are established risk factors.4
We report an exceptional case of delayed common femoral artery (CFA) perforation two months after primary uncomplicated THA for tuberculous coxitis, highlighting the need for vigilance beyond the immediate postoperative period.
Case report
Preoperative assessment
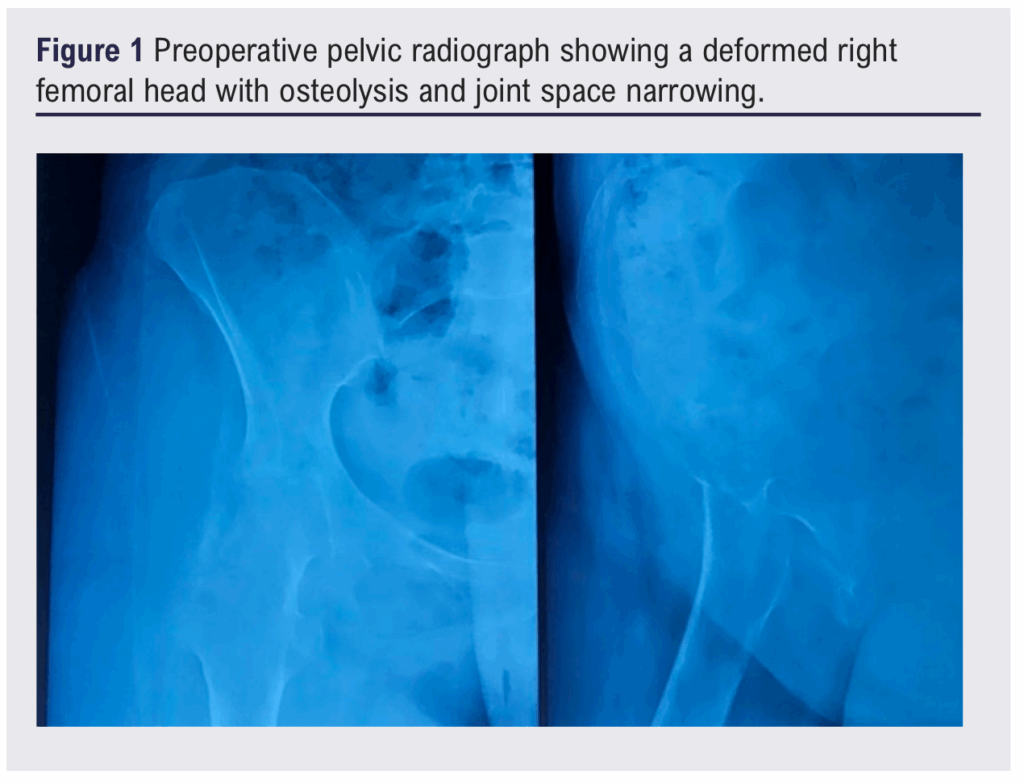
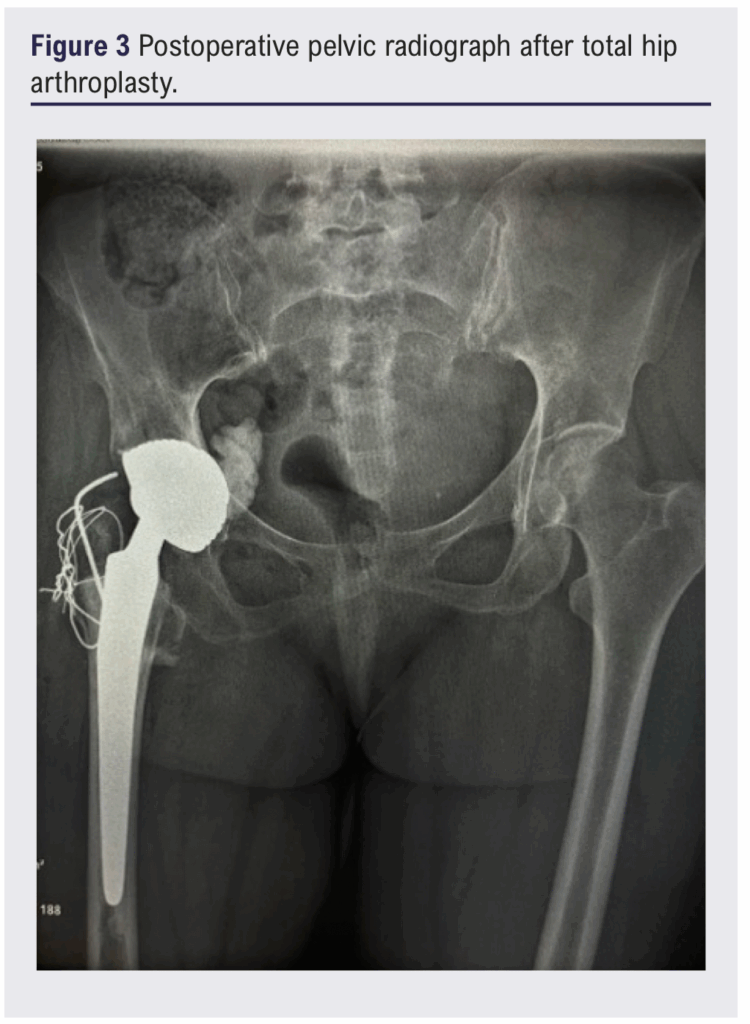
A 38-year-old woman with treated pulmonary tuberculosis presented with an 18-month history of right hip pain and limping. Examination revealed restricted flexion without vascular or neurological deficits. A pelvic radiograph demonstrated destruction of the femoral head and acetabular changes consistent with chronic coxitis (Figure 1). A CT scan confirmed chronic right-sided coxitis with muscular atrophy (Figure 2). Bone biopsy verified tuberculous infection. After multidisciplinary review she underwent THA using the Hardinge lateral approach. Intraoperative fluoroscopy was satisfactory and the early postoperative course was uneventful (Figure 3), with postoperative haemoglobin 9.6 g/dL.
![]()
Postoperative presentation
Two months later the patient developed sudden low back and groin pain radiating to the thigh. The hip was held in flexion; distal pulses remained palpable. Laboratory results showed severe anaemia (haemoglobin 4 g/dL). Because she was haemodynamically stable, surgical exploration was performed without preoperative angiography.
Operative findings and management
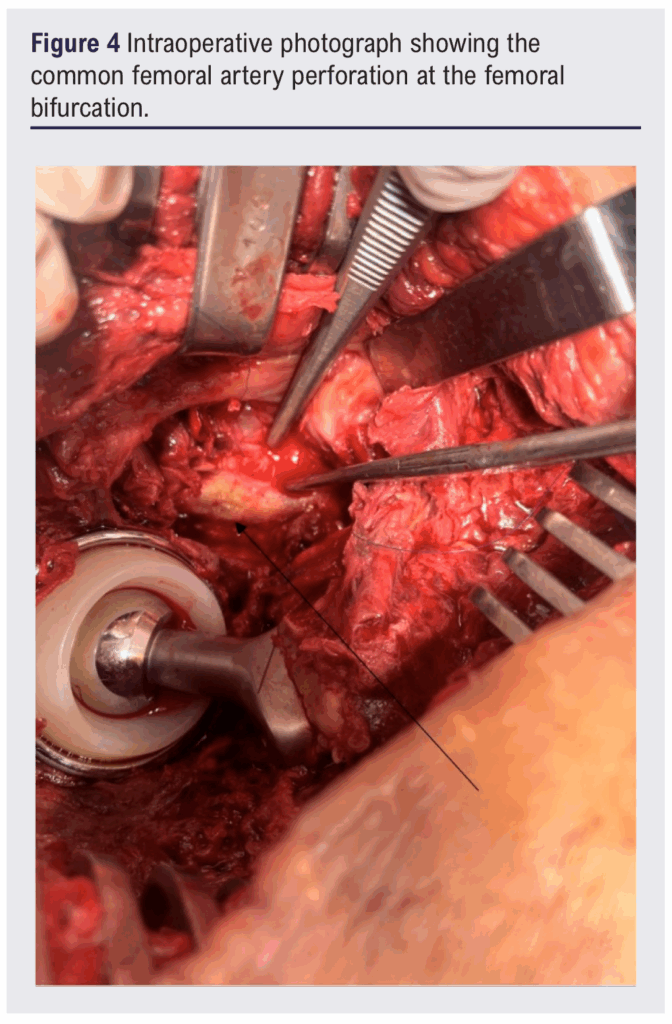
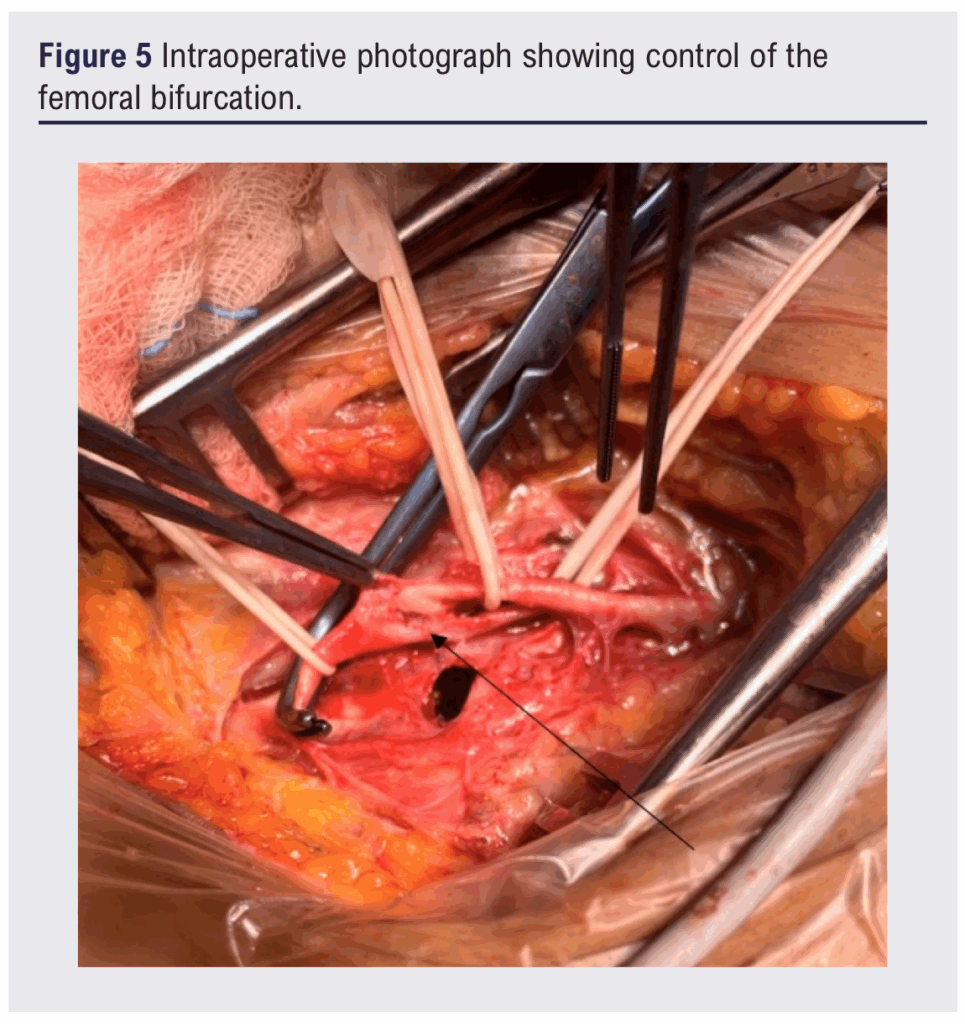
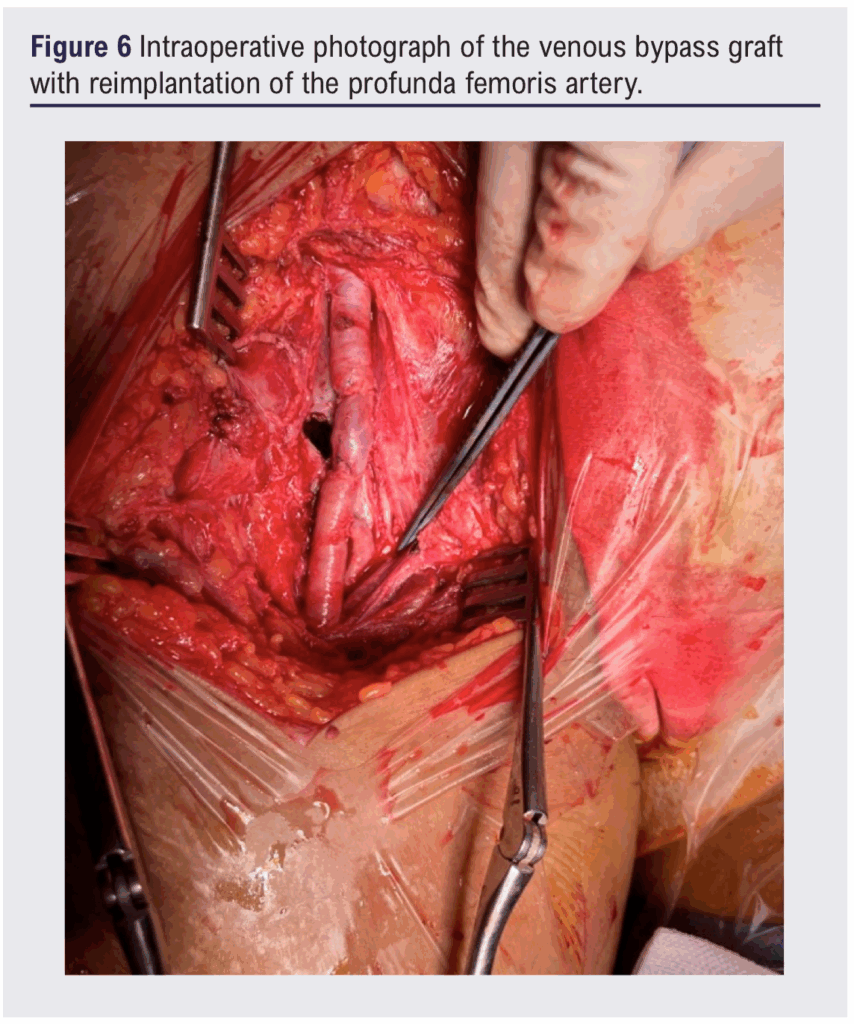
A large haematoma was evacuated, revealing active arterial bleeding at the femoral bifurcation. The vascular team was called. After proximal and distal control, a transfixing perforation of the CFA was identified (Figures 4 and 5). The damaged segment was excised and continuity restored with a reversed autologous saphenous vein graft from the CFA to the superficial femoral artery, with profunda femoris re-implanted into the graft (Figure 6). The patient recovered uneventfully with preserved limb perfusion.
Discussion
Vascular injury during THA remains rare yet potentially catastrophic. Reported incidence ranges between 0.2% and 0.42%.1 The external iliac and common femoral arteries are most often involved because of their proximity to the acetabulum and femoral canal.2 Early recognition is crucial, since delayed diagnosis can lead to limb loss or death.3
Mechanisms include direct trauma from retractors, drills or acetabular screws; thermal damage from bone cement; traction-related intimal disruption; and delayed perforation from pseudoaneurysm erosion.4,5 Our patient lacked traditional risk factors – no revision surgery, dysplasia, pelvic fracture or fibrosis – emphasising that even technically uncomplicated primary THA can produce vascular complications.
Delayed presentations, such as pseudoaneurysm rupture months after surgery, are diagnostically challenging. Collateral circulation may maintain distal pulses, masking acute ischaemia.6 Therefore, persistent groin pain, thigh swelling, neurological deficit or unexplained anaemia after THA should raise suspicion for vascular injury. CT angiography remains the diagnostic modality of choice when haemodynamic stability allows.
Management depends on lesion type and location. Endovascular therapy is increasingly preferred for contained perforations or pseudoaneurysms in anatomically suitable sites.7 However, open reconstruction remains essential when the femoral bifurcation is involved, when infection is possible, or when prosthetic artefacts limit imaging accuracy.8 Autologous saphenous vein provides durable infection-resistant reconstruction, as illustrated in this case.
This experience underlines the necessity of continued postoperative vigilance and close collaboration between orthopaedic and vascular teams. Even in primary THA, awareness of vascular anatomy, meticulous technique and prompt multidisciplinary action are vital to preventing devastating outcomes.
Conclusion
Common femoral artery perforation following THA is exceptionally rare but potentially life-threatening. Delayed presentation, as in this case, complicates diagnosis and management. Persistent groin pain, anaemia or neurological symptoms after hip arthroplasty should always prompt vascular evaluation. Early diagnosis and multidisciplinary collaboration between orthopaedic and vascular teams remain vital for limb salvage and survival. Preventive strategies include meticulous surgical technique, respect for anatomic variations and careful postoperative vigilance.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2025;5(1):34-37
Publication date:
November 17, 2025
Author Affiliations:
Department of Vascular Surgery, University Hospital of Tangier, University Abdelmalek Essaadi, Tangier, Morocco
Corresponding author:
Dr Ouassim Mouyarden
Department of Vascular Surgery, University Hospital of Tangier, University Abdelmalek Essaadi, BP 917, Tangier, Morocco
Email: [email protected]


")

")

