CASE REPORT
Spinal cord infarction due to immune thrombocytopenic purpura following aorto-bifemoral bypass surgery: a rare complication
Ragobar C, Sanadi C, Ghoneim B
Abstract
Spinal cord infarction is a rare but devastating complication following aorto-bifemoral bypass surgery, particularly in patients without typical risk factors. We report a unique case of a 68-year-old female who developed acute spinal cord infarction in the setting of newly diagnosed immune thrombocytopenic purpura (ITP) after undergoing elective aorto-bifemoral bypass surgery for chronic aorto-occlusive disease. Despite an initially uncomplicated procedure, the patient developed significant postoperative thrombocytopenia followed by profound neurological deficits. MRI revealed spinal cord infarction at the T11–L1 level. Haematological investigations suggested a paradoxical thrombotic event associated with ITP. This case highlights the need for heightened vigilance regarding thromboembolic risks in patients with ITP, even in the postoperative setting where bleeding complications are typically prioritised. Awareness of this potential complication is crucial for timely diagnosis and management.
Introduction
Immune thrombocytopenic purpura (ITP) is an autoimmune disorder characterised by the production of autoantibodies, commonly IgG, that target platelet surface glycoproteins (eg, GPIIb/IIIa), leading to platelet destruction primarily in the spleen. In some cases it also impairs platelet production in the bone marrow. Paradoxically, ITP can also be associated with thromboembolic events, including spinal cord ischaemia or infarction.1,2 Potential triggers for ITP include infections, autoimmune diseases, medications and post-trauma or post-surgery.
Aorto-bifemoral bypass surgery is a major procedure typically performed for aorto-occlusive disease. There is a paucity of reports describing spinal cord ischaemia in the context of ITP following this type of surgery.3 In aorto-occlusive disease, chronic stenosis or obstruction of the aorta and its branches leads to the development of collateral circulation to maintain blood supply to vital structures, including the spinal cord. However, these collaterals may be insufficient during acute occlusion, perioperative hypoperfusion or surgical disruption, potentially leading to spinal cord ischaemia. Spinal cord ischaemia has more commonly been associated with aneurysmal disease related to aortic aneurysm rupture and systemic hypotension.4,5
Case presentation
Patient demographics and preoperative details
A 68-year-old female, ex-smoker, with a background of peripheral arterial disease, previous femoral-femoral crossover bypass, hypertension and hypercholesterolaemia, presented with bilateral rest pain, worse on the left. Duplex and 3D CT imaging revealed occlusion of her previous graft. Visceral branches and bilateral internal iliac arteries were patient. Preoperative cardiac assessments showed adequate function with an ejection fraction >50% and 90% stenosis of the right coronary artery with stable angina. Preoperative platelet counts were normal, and she was deemed fit for aorto-bifemoral bypass surgery.
Surgical details
The patient underwent an uncomplicated aorto-bifemoral bypass via transverse laparotomy and bilateral vertical groin incisions using a 14×7 rifampicin-soaked Dacron graft. The proximal aortic clamp was placed infrarenally. The proximal anastomosis was done in an end-to-end fashion and was completed in approximately 25 minutes. Blood loss was approximately 1 L, and the minimum systolic blood pressure during surgery was 100 mmHg. The surgery lasted 5 hours and 45 minutes, reflecting the time required for careful aortic exposure through a transverse laparotomy and bilateral re-do common femoral artery dissection. Bilateral pedal pulses were restored postoperatively. Prior to surgery the patient received a spinal local anaesthetic block.
Postoperative complications
The patient remained intubated and sedated until postoperative day 2. Upon extubation she was confused (Glasgow Coma Score 14/15), and this confusion persisted for 2 weeks. Platelet counts significantly deteriorated over the first 4 postoperative days to a nadir of 18×109/L. Sepsis was ruled out (afebrile, negative blood cultures) and heparin-induced thrombocytopaenia was excluded with haematology input.
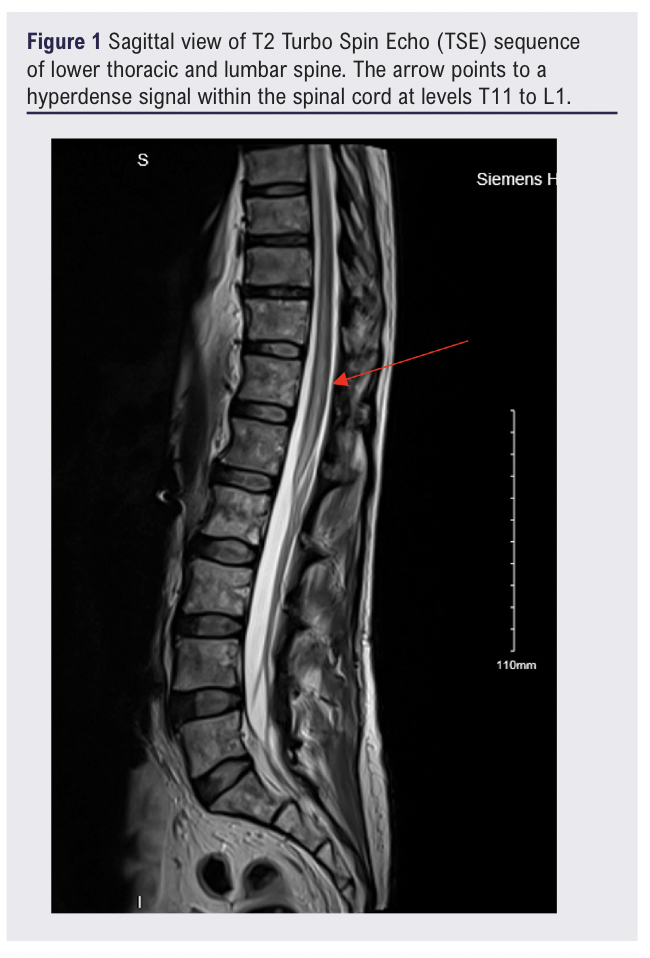
On postoperative day 4, new bilateral foot drop was noted. Neurological examination showed complete loss of power (0/5) and sensation in both lower limbs, absent reflexes and faecal incontinence. MRI on postoperative day 4 revealed acute spinal cord infarction from T11 to L1 involving the conus medullaris. This can be seen in figure 1 and figure 2. No haematoma was identified.

The neurology and haematology teams hypothesised that the spinal cord infarction was due to a paradoxical thromboembolic event in the setting of acute ITP.
Management and outcomes
The patient was treated with high-dose methylprednisolone for 5 days. She engaged in intensive rehabilitation. After a 3-month inpatient stay she had partial sensory and motor recovery but remained non-ambulatory. She was referred to a national rehabilitation unit.
Discussion
Spinal cord infarction is a devastating but rare complication of aortic surgery, more commonly associated with aneurysmal disease due to hypotension or extensive clamping.4,5 In occlusive disease, collateral circulation often provides protection, making spinal cord infarction after aorto-bifemoral bypass rare.
The spinal cord’s vascular supply includes the anterior spinal artery (supplying the anterior two-thirds) and two posterior spinal arteries. The artery of Adamkiewicz, usually arising between T8 and L4, plays a crucial role.6,7 Disruption to this artery or its collaterals increases the risk of infarction, particularly during high aortic clamping or compromised internal iliac flow.8,9 Typically, anterior spinal artery syndrome presents with motor deficits, urinary and faecal incontinence, while vibration and proprioception remain intact. MRI is the gold standard investigation. Management is supportive with rehabilitation.
Previous literature reports a very low incidence of spinal cord ischaemia after occlusive disease repair (approximately 0.3%).10 Spinal cord ischaemia after aneurysmal repair is more frequent.
Concerning ITP, while typically associated with bleeding, studies have shown increased thromboembolic risks.1,2 This paradox is believed to stem from platelet microparticles and immune-mediated endothelial activation.
To our knowledge, this is the first reported case of spinal cord infarction secondary to ITP following aorto-bifemoral bypass. The temporal association of sudden platelet drop, platelet transfusion and spinal cord infarction suggests a paradoxical thromboembolic phenomenon.
Other operative factors were considered but were unlikely, given the short clamp time, absence of significant hypotension and adequate systemic heparinisation.
Conclusion
This case highlights the need for heightened vigilance for thrombotic complications in patients with ITP, even after non-aneurysmal aortic surgery. Although rare, spinal cord infarction is a catastrophic event that must be recognised early. Understanding the thrombotic potential in patients with ITP can guide closer monitoring and early intervention.

Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2025;5(1):28-30
Publication date:
October 16, 2025
Author Affiliations:
Department of Vascular Surgery, University Hospital Limerick, Ireland
Corresponding author:
Claire Ragobar
Department of Vascular Surgery, University Hospital Limerick, St Nessan’s Road, Dooradoyle, County Limerick V94F858, Ireland
Email: [email protected]


")

")

