ORIGINAL RESEARCH
The ulcer with no fixed abode: barriers in accessing venous healthcare for individuals experiencing homelessness and using intravenous drugs in Bristol, UK
Bitterlin M,1,2,3 Clapp A,2 Simpson S,1 Curd C3
Plain English Summary
Why we undertook the work: People who are homeless and inject drugs have higher rates of cardiovascular (heart and artery) disease. There are currently no reported studies focused on venous (vein-related) disease, despite the risk of blood clots (deep vein thrombosis or DVT). DVTs can be deadly if left untreated. Damage to the veins is common in this patient group and can lead to chronic leg ulcers, pain, infection and swelling, which can be life-limiting and life-threatening. This is a health inequality and overstretching finite NHS resources. Diagnosis requires outpatient ultrasound scans prior to treatment (eg, blood thinning medication and/or surgery). These patients often do not attend these appointments, instead presenting at A&E with more critical health. This can result in delayed treatment, higher risk and greater NHS expense. Known barriers exist to accessing healthcare; however, the relevance of these to venous healthcare has not been explored previously. What we did: 15 individuals were recruited and interviewed in drop-in clinics in a charity and homeless GP practice in Bristol. Staff in these organisations have built rapport and are known to the participants so directed potential participants. Eligible participants had a history of venous disease, homelessness and injecting drugs. Semi-structured interviews were used to explore the barriers faced, which were then analysed into themes.
What we found: Five separate themes emerged: (1) competing priorities; (2) stigma; (3) practical barriers; (4) treatment limited to anticoagulation and/or compression stockings only; and (5) knowledge and understanding of own health. Barriers previously reported to healthcare utilisation also apply to venous healthcare including stigma, practical barriers and competing priorities to healthcare (eg, drugs or housing). Appropriate opioid substitution treatment (used to help individuals cope with withdrawal symptoms) reduces the need to earn money for drugs, which readjusts priorities towards healthcare. Specific barriers exist related to venous healthcare including: (1) venous ulceration and associated odour cause stigma and embarrassment; (2) treatment for chronic venous conditions is limited to compression with inherent barriers from required compliance; (3) harm reduction and homeless health services cannot refer individuals for specialist vascular review/imaging; and (4) poor knowledge in the target population of groin-related pathologies such as DVT contributes to delayed presentation.
What this means: Barriers exist to accessing venous healthcare with both acute (eg, DVT) and chronic (eg, ulceration) disease for individuals experiencing homelessness and using intravenous drugs. These barriers are exacerbated by poorly managed opioid substitution treatment. Venous ulceration causes stigma and embarrassment contributing to untimely healthcare utilisation. Treatment can be limited to compression and/or anticoagulation only and specialist vascular review/imaging cannot be requested directly by harm reduction and homeless health services. Vascular services need to consider how best to engage and serve this patient demographic to challenge this health inequality.
Abstract
Background: Individuals experiencing homelessness and using intravenous drugs are high risk for acute (eg, venous thrombosis) and chronic (eg post-thrombotic syndrome, ulceration, venous insufficiency) venous disease. Healthcare utilisation is erratic with known access barriers. This study sought to understand the relevance of these barriers in accessing venous healthcare by exploring lived experiences in Bristol, UK.
Methods: Participants with a history of homelessness, intravenous drug use and venous disease (n=15) completed a one-to-one semi-structured interview focused on lived experiences of accessing venous healthcare. Thematic analysis was undertaken, applying an interpretivist research paradigm.
Results: Five distinct themes were identified: competing priorities, stigma, practical barriers, anticoagulation/compression treatment only and knowledge of own health. Withdrawal symptoms present a daily burden, skewing priorities towards earning money for illicit drugs. Combined with previous stigmatising experiences, this results in delayed presentation until health is critical. The transient lifestyle of street homelessness conflicts with the traditional UK healthcare model of arranging/attending appointments. With this challenge of accessing primary healthcare, chronic venous conditions rarely result in referrals for specialist vascular review/imaging. Treatment instead focuses on anticoagulation for thrombosis and compression therapy for ulcers; both have inherent barriers from long-term compliance requirements. Acute and chronic venous disease are poorly understood by this population.
Conclusion: Participants described inequitable access to venous healthcare. The barriers faced are comparable to general healthcare utilisation, but with specific barriers to venous healthcare. Individuals are heavily reliant on community-based homeless health and harm reduction services and face challenges accessing specialist vascular services.
Introduction
Unstable housing is a growing UK issue with 178,000 households assessed as homeless in 2023–24.1 Health inequalities exist for this population,2 with untimely healthcare utilisation often via Accident and Emergency (A&E) when health is critical resulting in long periods of inpatient care,3-5 higher mortality,2 National Health Service (NHS) financial strain6 and ‘tri-morbidity’ (poor physical and mental health with substance abuse).7
Intravenous drug use (IVDU) has a higher prevalence in homeless individuals,8-10 reported in one study in 78% of individuals with a life history of homelessness.11 Groin injection is the most common access site,12 with long-term injection leading to sinus formation – a hole in the skin and subcutaneous tissue allowing direct venous access.13 This reduces the risk of ‘missing a hit’,14 but also allows discretion from the public, family members or police,12 perhaps explaining higher rates of groin injection with individuals experiencing homelessness.15
Femoral vein damage occurs in the vast majority of individuals who groin inject13 due to various mechanisms detailed elsewhere.11,15–17 Deep vein thrombosis (DVT) is reported to be three times more common with femoral injection,12 and long-term damage results in venous insufficiency13,18 and leg ulcers.3 A general lack of uniformity is reported in treating longstanding venous disease in this population.19
Improved prevention and/or treatment of chronic conditions such as ulceration may save individual suffering and costs to the NHS;20 however, barriers to accessing diagnostic/treatment pathways need to be established. There are currently no qualitative studies focused on the barriers for this population accessing venous healthcare. Venous healthcare is multifaceted, with diagnostic and treatment pathways including but not limited to duplex assessment for acute DVT, ulcer assessment, prescription of compression hosiery, duplex assessment for venous incompetence/insufficiency and venous intervention (eg, deep venous recanalisation, foam sclerotherapy, radiofrequency ablation). The barriers to accessing healthcare in general have been explored in previous qualitative research based in Australia,8,21 Canada,22,23 Ireland,24-26 the Netherlands,27 the UK28 and the USA.5,29,30 A range of themes have been described including stigma,5,6,21–23,25,28,30 practical barriers,21,24 poor adherence to treatment6,8,26 and chronic pain being a low priority concern.22 The aim of this research is to explore the relevance of these and other barriers in accessing venous healthcare (diagnostics and/or treatment) from service users’ perspective.
Methods
Research methods
This qualitative research used interviews and thematic analysis applying an interpretivist research paradigm.31 The Principal Investigator was in-post locally as a Trainee Vascular Scientist, thus arriving at the research with biases based on interacting with the target population in an acute hospital setting for vascular ultrasound investigations.
Ethics
Health Research Authority (HRA) and Research Ethics Committee (REC) approval was obtained via the Integrated Research Application System (IRAS) (ID 342033). Newcastle University approved and sponsored the project.
Recruitment
Recruitment used non-probability sampling methods. Convenience and purposive sampling were used as defined by Stratton.32 This approach was adopted due to transient nature of the individuals using intravenous drugs and experiencing homelessness. Traditional recruitment methods of contacting via post and telephone were not viable with this population due to the challenge of having no fixed abode or telephone number. Recruitment took place at Bristol Drugs Project (BDP), a charity providing harm reduction services, and The Compass Centre, a BrisDoc Homeless Health GP practice. These venues were used for ease of participant access with specialist staff available on site for medical, emotional, social and safeguarding support if required. The Principal Investigator was based in these venues for a two-week period in November 2024. Local staff in these venues acted as gatekeepers and directed potential participants from drop-in clinics to the research team. The Principal Investigator explained the study using a Participant Information Sheet and potential participants who met the inclusion criteria were consented by the Principal Investigator who obtained informed written consent using a consent form. Participants were renumerated with a £10 cash stipend. Light refreshments were provided during the interview. A research grant was awarded by The College and Society for Clinical Vascular Science (CSVS) to cover transcription and stipend costs.
Sample size
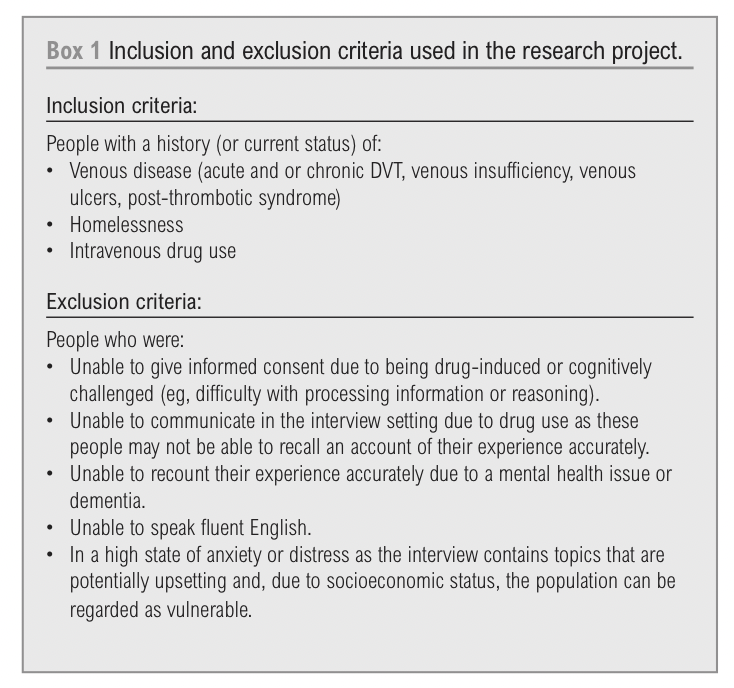
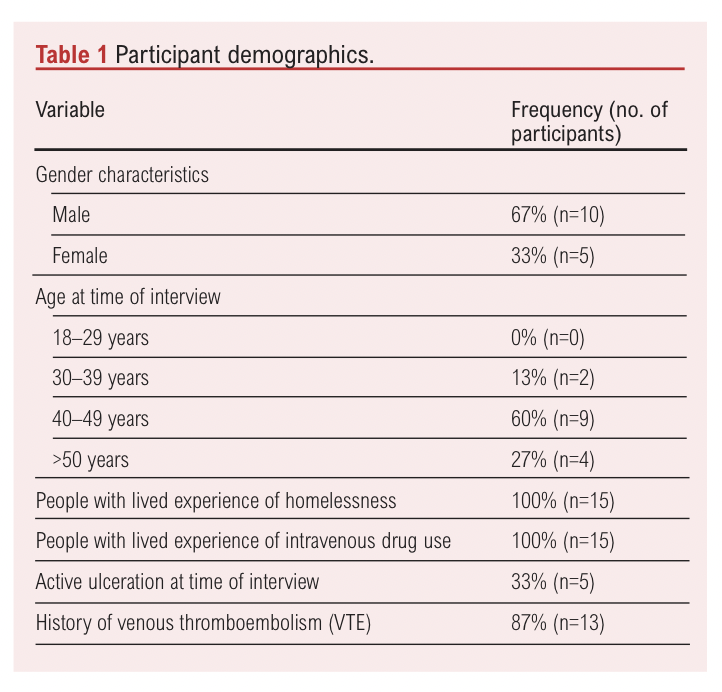
An initial sample size of 10 was planned for and was extended to 15 due to early success with recruitment, at which point data saturation was reached and recruitment ceased. It is not normal practice to complete a power calculation for qualitative research, so this sample size was chosen in line with other similar qualitative studies as well as pragmatic considerations of the time scale of the project as it was completed between September 2024 and May 2025. The inclusion and exclusion criteria used in the research project are shown in Box 1 and the demographics of the participants are shown in Table 1.
Data gathering
Participants completed a one-to-one face-to-face semi-structured interview about their experiences (mean length of time 32 minutes). Interviews occurred in the host venues concurrently with drop-in clinics for participant convenience. An interview schedule was used with open-ended questions in a semi-structured manner, allowing for discussion to emerge. The questions were written and refined based on themes explored within the literature review, casual conversations with host venue staff and consultation with the Bristol Drug and Alcohol Health Integration Leadership Team. Follow-up questions were asked as required to expand/elaborate on points, opinions, thoughts and/or feelings. The interview schedule evolved throughout the interviews influenced by the interactions of the researcher with the participants and casual conversations with staff in the host venues. Interviews were audio-recorded and outsourced for transcription (UK Transcription).
Data analysis
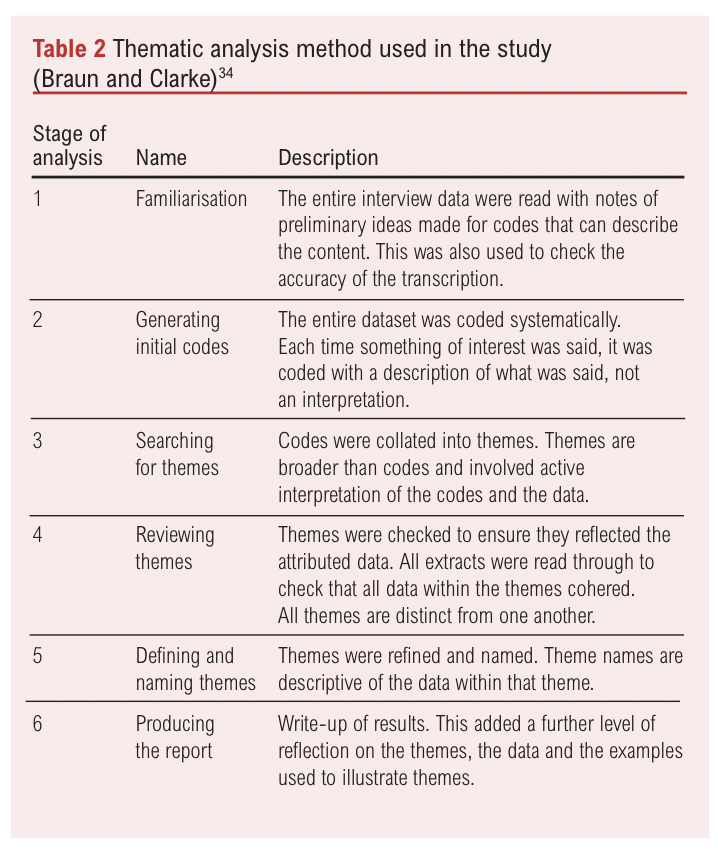
The data were handled using NVivo 15 software33 and thematic analysis was undertaken applying the Braun and Clarke method (Table 2).34 The coding method was data-driven with codes systematically assigned by the researcher, which were then formulated into sub-themes. Reflexivity was practised throughout the coding which took place over several weeks and the content was discussed with members of the research team experienced in quantitative research. Over time the codes were grouped into sub-themes and commonality was established to name the overall themes. These were further refined to ensure the name of the theme accurately reflected the sub-themes assigned. The assignment of themes would have been influenced by the biases of the Principal Investigator working in post within a diagnostic vascular laboratory and reflected on throughout the process. Unfortunately, it was not possible to undertake triangulation validation as analysis was undertaken solely by the Principal Investigator as part of an MSc level award. Participant validation was attempted but was not possible given project time constraints and the transient nature of individuals experiencing street homelessness.
Results
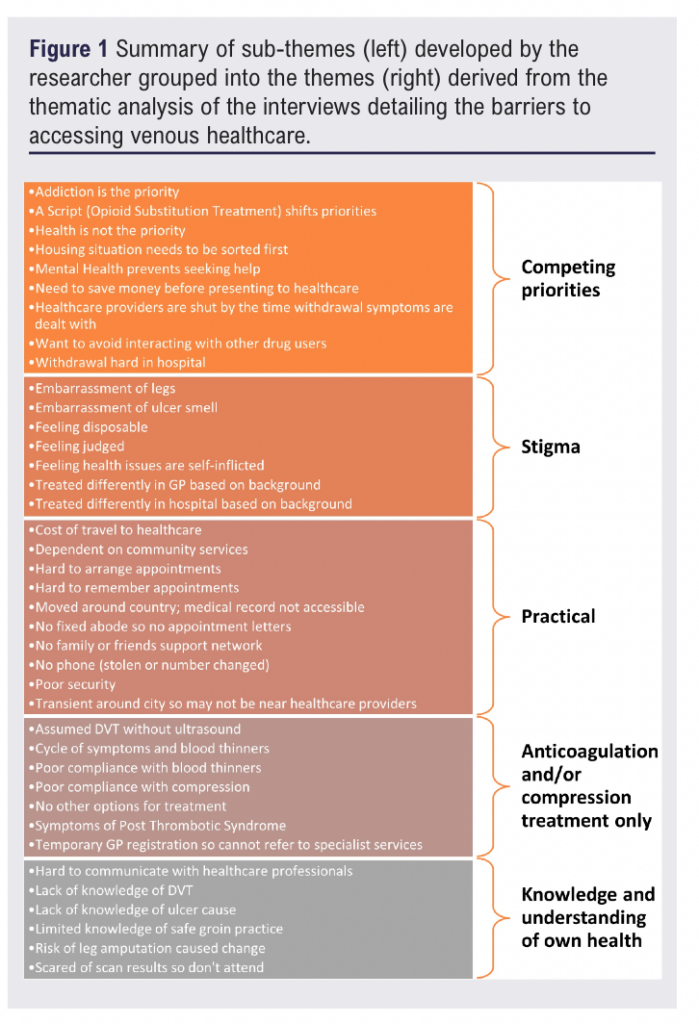
Sub-themes were grouped in commonality by the Principal Investigator to form five separate themes. These themes are distinct from one another and centre around the research question. The overall thematic analysis findings are shown in Figure 1 with a more detailed breakdown below.
Competing priorities
Competing priorities describes the need for individuals to deal with other daily concerns deemed more important than health concerns. This centres around the need to earn money for a variety of needs including food and drugs as well as gain stable housing.
Competing priorities was a significant barrier to presenting to healthcare, particularly as addiction was always the main priority:
“When you’re in that addiction state, that’s the only thing that matters.”
To serve this addiction, all participants described waking up each morning with a focus to ‘get well’ – a common expression used for alleviating withdrawal symptoms:
“That was the main priority of the day (getting well). Once I’d dealt with that, then I’d deal with my health and everything comes later.”
Getting well required working to earn money for drugs including begging, shoplifting, prostitution or dealing. This commonly took all day to earn enough money meaning health was the last priority and could often only be dealt with once primary healthcare was closed:
“Your time just gets consumed when you’re homeless … you’re going out and begging for money and stuff … you need to get well before you do anything …. So, you spend the whole day trying to get well. By the time you’ve done it, everything’s shut.”
This situation is made worse when struggling with venous ulcers:
“Wake up in the morning, sheer panic … you’re getting the usual withdrawal symptoms … you’re broke and you’re sore, you can’t move, and especially when you’ve got f****** ulcers because that makes the pain twice because your pain threshold has gone … Then, all of a sudden, you wake up and think, “Oh, I need help … it’s all shut, I can’t do it. I’ll do it tomorrow” and, of course, it gets worse and worse and worse.”
One participant described an extreme experience of this with reduced sensitivity to pain from opioid use resulting in their venous ulceration progressing down to the bone before presenting to healthcare. Multiple participants talked about peers who had lost limbs or lives due to delayed healthcare presentation caused by this daily cycle. Even when health became critical, some participants would still wait to attend A&E:
“I’d always try to hold out until it was my payday because I never wanted to go in there with no money, with no cigarettes and stuff like that, and rely on people.”
Several participants explained the severity of withdrawal symptoms as an inpatient leading to self-discharge before completion of treatment or forcing discharge by refusing treatment to deal with their addiction.
Symptoms of post-thrombotic syndrome (PTS) were described with chronic intermittent lower limb pain and swelling following DVT. PTS occurs due to the associated damage to the valves and veins caused by a thrombotic event in the affected limb resulting in chronic venous insufficiency. The daily need to ‘get well’ meant there was no time to alleviate these symptoms through rest, exacerbated by the transient nature of street homelessness:
“You’re not able to settle in a place or be settled long enough yourself, because you need rest, you need nutrition, you need to have to sit down and be able to heal, you need to be able to elevate your legs.”
All participants talked about ‘a script’ referencing prescribed opioid substitution treatment (OST). OST includes prescribed replacement opioids such as methadone and buprenorphine, which are used to support withdrawal from opioids such as heroin. With appropriate OST, health could be addressed during primary care opening hours and reinstated as a priority from the reduced need to ‘get well’.
Housing was an area of significant concern for many and particularly those living on the street at the time of the interview. Attending housing meetings, applying for housing or securing a hostel for the night were all described as higher priority than health. There was a perception by those in this situation that, if their housing situation were improved, health could then be prioritised
“I’m bidding on Home Choice. I’m really close to … getting my own council property, and when that happens, my life’s
going to change massively because … with a home … I can look after myself better.”
However, housing comes with the financial pressure of rent that can trap individuals in a cycle due to unsustainable rental costs. This can result in healthcare remaining a low priority concern:
“I’m a qualified chef … I’ve always had opportunities. If you go and get a job, if you’re at Salvation Army, they let you
have four weeks free … but after that you’re then liable for the £330 a week rent and the £125 a month service charge. So that’s £1445 … without paying for food.”
Mental health (including low self-esteem, depression, bipolar disorder, psychosis and ADHD) was also described as a competing priority over physical health, with participants associating this with an ability to engage with healthcare professionals. This made it challenging to attend outpatient appointments as well, with several individuals describing situations where they feared leg amputation if they presented to healthcare.
Stigma
Stigma relates to the treatment participants received based on their background as an individual experiencing homelessness and using intravenous drugs. This feeling and fear of stigma can be due to previous interactions with healthcare providers and a general feeling of embarrassment for presenting to healthcare with self-inflicted concerns. Individuals described severe stigma in society ranging from parents shielding children from this population in the street, abusive language/behaviour and, in some instances, this was so extreme with being woken up on the street, being urinated on or set on fire. Participants spoke passionately about healthcare being a place of safety and this makes stigmatising behaviour in healthcare providers even more degrading.
Stigma was referenced by all participants commonly manifesting in different treatment based on background:
“They don’t treat you the same (if you’re an addict) … as a normal person.”
Stigmatising attitudes can be overtly apparent as soon as healthcare staff realise IVDU status:
“I’ve gone into the hospital … and they’re talking to me … and they’re all chirpy and that … then the tone of voice just completely changes and the whole demeanour changes. It’s almost like they’ve taken it to a personal level to basically deflate you by saying certain things that are quite hurtful and painful.”
Late presentation to healthcare results in being seen in A&E with lower limb venous symptoms and the stigma of IVDU often results in long A&E waits:
“You’re sat six hours waiting to be seen by the triage, when someone else would come after you and you’re still waiting … and they talk about you in the back … but we can hear … it’s like they’ve got no time for people that do drugs, to be honest.”
While appreciation of systemic long A&E wait times was mentioned, many associated their treatment with their background:
“And I do believe, I’ve got absolutely no evidence that it’s intentional, but when you’re going into A&E and you’re waiting seven hours, and just about everybody else is coming in and getting seen in four … Your head’s going to tell you it’s intentional and there’s a judgement being made on you because of what you’re in for and because of your status as a homeless person.”
Participants described giving up after several hours and walking out. The experiences of individuals who waited were quite negative including stigma during an ultrasound scan for DVT:
“As soon as I mentioned that it’s through an old drug addiction, like I just saw the lady’s face (who was completing the
ultrasound scan) go from a smile to upside down to a frown. She just wanted me out of there.”
Stigmatising behaviour could be so overt that participants could be refused a same-day diagnostic ultrasound scan for DVT:
“ ‘Yeah, it could be a clot’, and this is no word of a lie, you can ask my keyworker, the doctor turned round and said … ‘But you’re a drug user, you have to come back tomorrow’.”
Multiple participants described lack of privacy in hospital – for example, when showering or toileting due to perceived staff suspicion of opioid use. One participant described how curtains needed to remain open with visitors requiring identification. An overriding sense of not being listened to and feeling worthless was portrayed, shown in this extreme situation a week prior to the interviews:
“I pressed the buzzer. In the time that I’d pressed the buzzer, I managed to hang myself, snap the sheet, and still it was
about an hour and a half from the time I pressed the buzzer to the time they answered it.”
Participants explained that, when an individual attends hospital, they are desperate for help but then feel judged. Individuals perceive staff are trying to oust them. However, focused efforts are needed to give as much help as possible before discharge:
“And when you’re in hospital, it’s that situation, I think there’s a lot of people that think what they’ve done is just such a shock that they’ve ended up in hospital because of it, they’re like, ‘S***, now I’ve got to stop’. And that’s when you need to get them.”
Treatment pathways were often described as different due to individual background. One participant described how staff thought they were lying about pain scores to be given opioid pain therapy while another described waiting for several hours in A&E before receiving any pain relief. Stigma can remain when using healthcare despite being clean for several years:
“You’re looking at my records and you’re judging me because I was an addict. I see you looking at my notes, I see the alerts, I know what they mean. If you’re not willing to offer me the same pain pathways that you would offer to a regular person, then I need to speak to your practice manager, because you’re discriminating against me because of my past.”
Stigma of using intravenous drugs also then combines with embarrassment, which was a commonly used term particularly associated with chronic leg changes: sinus formation, oedema, discolouration and varicose veins. Individuals felt judged entering general practitioner (GP) practices or using public transport for appointments with the smell of venous ulceration. One participant detailed an extreme example of not leaving their hostel for four years in the longest stretch due to embarrassment, eventually presenting with whole leg, maggot-infested ulceration. Several participants explained how this stigma linked with a feeling of issues being self-inflicted:
“It’s the embarrassment side of it as well because I hate going to hospitals when it’s drug related because I feel so ashamed. This is my fault. I’ve done this and I’ve found it hard taking up a hospital bed that could be used for someone, you know, like a pensioner with COVID or childhood cancer, you know, whatever.”
Practical
Practical barriers relate to the logistical aspects linked with arranging and attending healthcare appointments as an outpatient. These include barriers such as lack of fixed telephone number, no fixed address to receive appointment letters and unknown distance to healthcare providers due to transient movement around the city.
All participants referenced a variety of practical barriers. Lack of family and/or friends support network was most referenced linked with attending outpatient appointments or having encouragement to seek medical attention. Consequently, participants relied on support workers to schedule, remind and physically take them to outpatient appointments. The situation would be different without a support worker:
“I’d be f*****. But now, because … I’ve got a mental health worker, I’ve got people behind me, they’re ringing me up every day, make sure I know about this appointment.”
There was a reliance on community services explained, including but not limited to the interview host venues. Individuals with active venous ulcers explained how community nurses linked with the Homeless Health Service visited them regularly in temporary accommodation for wound cleaning and dressing. Participants often had multiple concurrent appointments at the time of interview to collect OST, blood thinning medication, ulcer assessment/ redressing and/or have compression bandaging fitted. This was also coupled with appointments regarding housing and safeguarding. Hospital and GP outpatient appointments were described as more challenging due to set time/date requirements, focus on only one aspect of health and lateness resulting in refused consultation/treatment. Flexible appointment structures comparable to drop-in services in the host venues were valued by participants:
“They advise you. They give you information that you never knew … Same day scripts and stuff like that. They help with benefits here … They even help with housing. They’ve got nurses here, doctors here … I would say this place is a lot better for people living on the streets because they’ve got everything here that you require. Even sleeping bags … and they don’t turn you away … Whereas if it was the doctors’, it would be like you have to ring up and make another appointment, which could be in a week’s time.”
Wider practical barriers included not being contactable via telephone due to poor security and numbers frequently changing. This presented challenges for arranging appointments and/or receiving letters/results (sent via Short Message Service (SMS)). Physical letters often do not arrive due to temporary, absent or inaccurate address records resulting in missed appointments. Individuals can move around the country, and one participant explained how their medical records were inaccessible to local services leading to a breakdown in the continuity of care. Some participants mentioned how the transient movement around the city when experiencing homelessness gave uncertainty of distance to healthcare providers, exacerbated by difficulties walking with pain, swelling and ulceration.
Anticoagulation and/or compression treatment only
This theme related to treatment for participant’s venous disease and how this was limited to anticoagulation for episodes of acute DVT and compression hosiery for ulceration. Both require long-term compliance to have effectiveness, which brings inherent challenges for this population.
Participants described anticoagulation for DVT treatment, which is usually diagnosed on ultrasound. Diagnosis for this population was sometimes based on medical history alone, therefore acute DVT was assumed without ultrasound confirmation:
“Like, it would be because I’ve been IV using recently so, “Oh, it must be that so we’ll just whack you back on blood thinners.”
Even with ultrasound diagnosis, treatment often focused on a cycle of resolving acute DVT alone, which participants had frustration over.
“It’s always, like, scan, ‘No blood clot, blood clot, blood thinners, f*** off’, and that’s it.”
PTS symptoms were described yet none could recall discussion or investigation into this. Anticoagulation varied with some individuals on lifelong prescription and others on 6–12-month cycles based on symptoms.
It was clear that participants found long-term anticoagulation a burden as it was challenging to remember to collect prescriptions and, even if they were collected, individuals would just accumulate them and not take them. Individuals struggled to articulate why, but it was a recurring scenario. Some individuals showed a lack of understanding of why they were on long-term anticoagulation if the blood clot had resolved. Poor compliance led to resurgence of symptoms, which may warrant appointments and ultrasound scans starting the cycle over again. There were some more emotive reasons for not taking anticoagulation including self-harm bleeding risk and continued IVDU bleeding risk:
“When I was still f****** banging up [injecting] in my groin, I didn’t want to take them then, as well, because I am a bleeder anyway.”
Those with chronic symptoms such as venous ulcers described similar frustration with the compliance required for compression hosiery. Some of the participants in this study were engaging in healthcare by attending the host venues for compression and dressing changes yet arrived with their legs wrapped in plastic bags. Compression was described as cumbersome and uncomfortable so would often be cut off by the individual before the next appointment. Compression was generally described as effective, with individuals adamant that it would help their ulcers but having to attend regular appointments (2–3 times a week) for over a year provides a significant barrier to individuals who already struggle to attend appointments. This compression treatment was provided in the host venues and associated nurses who visited hostels daily to perform wound cleaning and dressing.
Knowledge and understanding of own health
This theme relates to a lack of understanding to identity key symptoms, which can result in delayed presentation. Most health knowledge in this population is shared on the street and gathered through experience. Several participants explained how there was a general lack of DVT knowledge resulting in delayed presentation:
“I didn’t think it was that bad, because I didn’t really know much about it. I don’t know much about DVT. I’d never really heard about it. So I never really knew about it.”
Only following initial diagnosis did individuals better understand DVT symptoms and when to seek medical help:
“I know, more, what to look out for now as well, like any sort of swelling, any sort of redness, any sort of pain, any uncomfortability [sic].”
It was suggested more drop-in services focused solely on groin/leg health including DVT would raise awareness:
“No, leaflets are no good … There should be some form of drop-in advice centre. Just somewhere that you can go.”
Several participants talked about safe groin injecting practice due to the proximity of the artery, nerve and vein. A lack of knowledge of the key symptoms linked with different pathologies (eg, DVT versus false aneurysm versus abscess) provided uncertainty of when/where to seek help:
“There’s no handbook written like say, ‘If this happens go to this, if this happens do this, if this happens do this’.”
Limited knowledge of ulcer causes was also found even if the individual had been suffering for several years, with none of the participants asked able to explain why they had an ulcer. Some were obviously perplexed that their ulcer had appeared years after groin injection. Many participants (n=5) mentioned the risk of leg amputation acting as a catalyst for healthcare utilisation:
“I didn’t want to lose my leg because of running around playing with her and stuff like that. I didn’t want to be the daddy that was crawling around to see my daughter.”
An inability to communicate with healthcare professionals was described with support workers relied upon to explain medical conditions/notes:
“They [healthcare staff] wouldn’t really sit down with me and explain what this meant … The only person who’d do it was … the drugs workers. I’d say to them, ‘Do you know what this means or that means?’ … I’m not from a medical background so I don’t really understand a lot of like … I’ve got dyslexia as well, so reading writing can be quite difficult.”
Discussion
Individuals experiencing homelessness and using intravenous drugs face barriers in accessing venous healthcare. Some of these are comparable to general healthcare utilisation including stigma, competing priorities and practical barriers. There are barriers specific to venous healthcare – notably, the embarrassment of ulcers, the inability to refer patients for specialist vascular review/imaging, a lack of treatment options available for chronic venous conditions (ulcers, PTS and venous insufficiency) and a lack of DVT knowledge prior to diagnosis.
Competing priorities
Competing priorities provide a significant barrier to accessing venous healthcare, with participants describing how addiction takes priority. Harris35 describes this as a ‘cyclic dynamic’ to obtain illicit drugs. Whilst other studies draw attention to different daily priorities akin to Maslow’s Hierarchy of Needs,8 this sample focused solely on the concept of ‘getting well’. Klop et al27 describe a daily survival mode, which participants recounted during times of severe addiction. Consequently, multiple participants attend A&E when health is critical – a common pattern of healthcare utilisation in this population.24
PTS does not feature in the wider literature; however, these symptoms were described by most participants. PTS-associated pain and ulceration increased the risk of further damage through IVDU for pain relief purposes. O’Carroll and Wainwright24 describe continued injection around ulcers, as mentioned by several participants. Comparable with previous findings, participants conveyed that repeated groin injection is due to ease of access, public discretion12,15 or lack of other access sites.14
Mental health featured heavily as a competing priority to venous health, with equally harrowing suicide attempts detailed by Harris.35 Cornford et al3 and Harris35 both describe how fear of leg amputation prevents presentation; however, this sample described the risk of acute limb loss as a catalyst for behaviour change.
OST reduced the pressure to ‘get well’ resulting in readjusted priorities towards healthcare. Lewer et al4 found that appropriate OST significantly reduces the likelihood of A&E presentation. Multiple participants described ineffective inpatient OST management, as previously reported;3,24,35 presentation would be delayed by waiting for payday to serve addiction whilst admitted, as found by Harris.35 Harris et al36 highlight the national inpatient OST inconsistencies, with severe bureaucracy limiting timely intervention. This contextualises participant descriptions of leaving A&E after waiting hours for pain relief or OST.
Attempts have been made to standardise hospital OST approaches and reduce this barrier; however, strategies can exacerbate feelings of stigma and mistrust – for example, point-of-care urine testing.37 Stigma has been described in relation to OST status due to the implication of addiction.5,30 Participants did not mention this, perhaps due to a degree of acceptance embedded from long-standing IVDU history.
Stigma
Stigma towards participants featured heavily and provided a significant barrier to presentation. Participants described being treated differently in healthcare based on IVDU status even if this was historic, which is widely reported.5,24–26 Stigmatising healthcare language is often used in medical notes rather than neutral person-first language,37 thus influencing staff preconceptions.30 Gilmer and Buccieri22 highlight how staff demeanour changes upon realisation of IDVU; comparable examples feature in this sample. Participants suggested this treatment was worse in the city centre hospital than in suburban hospitals. This may be linked to compassion fatigue as described Dowdell et al29 following years of dealing with acute withdrawal cases due to the comparative ease of access to the city centre hospital. As the skewed priorities of this population do not conform with norms of self-care,35 perhaps staff cannot relate to the individuals’ situation resulting in compassion fatigue. Subsequent care is not trauma-informed, and participants spoke about being made to feel their venous health issues were self-inflicted. Trauma-informed harm reduction techniques should consider the reasons for IVDU, emphasising that substance abuse is a health issue, not a moral failure.23–25,28 Ultimately, individuals are presenting to A&E in times of desperation and then negative stigmatising experiences with poor continuity of care degrade trust.21,25,28
Poor continuity of care was described by the participants, especially those in unstable housing. For some participants housing was a higher priority than health, as described by Harris.35 O’Donnell et al26 associate this situation with current homelessness or sex workers. Due to bed shortages, UK hospitals are pressurised to discharge medically fit individuals with inadequate provision for continuity of care such as OST.37 Participants describe lack of continuity in anticoagulation when diagnosed with acute DVT, and Harris35 highlights the lack of holistic support provided on discharge. Anticoagulation treatment pathways for DVT lack uniformity,19 concurring with this sample. Unsurprisingly, these factors lead to erratic compliance with medication,38 especially in instances of repeated PTS-like symptoms.3
Anticoagulation and/or compression treatment only
Gilmer and Buccieri22 report overemphasis on prescribing medication compared with other treatments. Similarly, this sample reported prescribed anticoagulation without appropriate ultrasound investigations to diagnose DVT. The long-term compliance requirements of anticoagulation and/or compression treatments present inherent barriers for this population.6,8,26,39
Participants struggle to be referred to specialist vascular services; a comparable finding with oncology35 and cardiology.6 Permanent GP registration is required. However, this sample described how they are ostracised in GP practices, a view in agreement with Armstrong et al28 who detail instances of refused registration.
Venous health has associated embarrassment that acts as a barrier.3 The most intense feelings of embarrassment are reserved for the smell of leg ulceration and abscesses,35 debilitating daily life. This shame and embarrassment has been reported in studies involving district nurses visiting hostels28 and pharmacy-based needle exchanges.5 In contrast, participants spoke highly of the host venues and associated nurses who visited hostels for wound cleaning and dressing. Care provided in these community settings was always described as non-judgmental, in keeping with Armstrong et al.28
Practical
Practical barriers corresponded with previous studies including time poverty due to other commitments,35 transient movement causing geographical access issues21 and difficulties accessing medical records with address changes.6 Purkey and Mackenzie23 suggest that the presence of an advocating support worker significantly improves the quality of healthcare delivered, although this was not specifically mentioned in this sample. Participants instead emphasised the necessity of a support worker in scheduling, reminding and physically escorting individuals to appointments. Participants were extremely complimentary of the care provided by the host venues, reiterating the need for drop-in services in community settings8 with suitably trained professionals who are easily approachable to build trusting relationships.27
Knowledge and understanding of own health
Previous studies have shown the value of access to diagnostic ultrasound scans in familiar community settings.13 While not directly described by participants, the inherent barriers of attending appointments in hospital have already been discussed. Consistent with Cornford et al,3 participant knowledge of DVT symptoms was limited prior to initial diagnosis. O’Carroll and Wainwright provide comparable examples of delayed presentation caused by uncertainty of DVT symptoms.24 Participants described self-care of groin-related issues until symptoms were unbearable, which Robertson et al40 associate with progressive and cumulative damage. Participants lacked knowledge of ulcer causes, which may link with Coull et al20 who relate misdiagnosis with inappropriate use of antibiotics due to assumed infection rather than addressing underlying venous issues. This is despite venous insufficiency reported in 55% of one sample of groin injectors.13 Consistent with Coull et al,20 this sample described how chronic venous issues occurred long after ceasing IVDU. Doran et al39 positively associate venous insufficiency with >15 years of IVDU.
Strengths and limitations
This is the first study to focus solely and directly on the barriers to venous healthcare from the perspective of individuals experiencing homelessness and using intravenous drugs in the UK. The findings may be transferable to similarly marginalised individuals in the UK and globally.
The findings are not generalisable as typical with qualitative research design and are limited to a specific social context of select individuals experiencing homelessness and using intravenous drugs in Bristol, UK. The findings may have reduced validity due to lack of analysis triangulation or participant validation. The findings represent solely one perspective and further insight would have been gained by interviewing healthcare or other independent professionals (eg, support workers), but this was beyond the scope of this research. The individuals recruited in this study were actively interacting with healthcare and/or harm reduction and therefore the views of individuals not interacting with these services may differ.
Conclusion
Individuals experiencing homelessness and using intravenous drugs in Bristol, UK are a marginalised group with unequitable access to venous healthcare compared with the wider population. The barriers faced are comparable to general healthcare utilisation. Some of these barriers are very specific to venous healthcare, such as the daily life-limiting stigma of venous ulceration, the lack of care consideration for chronic venous conditions and poor knowledge and understanding of groin-related pathologies. Individuals depend on the specialised harm reduction, homeless health and support worker services due to the barriers faced in accessing the traditional UK healthcare model. This study provides a useful insight into how these barriers present for individuals, albeit in a small study specific to one particular geographical area and is therefore not generalisable. Further research in this underrepresented area is required, with larger studies to establish the transferability of these findings and in doing so should consider how these barriers can be addressed. The inability of local harm reduction and homeless health services to refer individuals to specialist services such as Vascular is particularly concerning and would be a meaningful future research or service improvement area of focus. Equally, no studies exist to date that document the extent of chronic venous disease in this population, and quantifying these may serve useful in understanding the scale of this issue in a very underrepresented and underserved group suffering blatant health inequalities.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2026;5(3):134-144
Publication date:
May 27, 2026
Author Affiliations:
1. University Hospitals Bristol and Weston NHS Foundation Trust, Bristol, UK
2. Newcastle University, Newcastle upon Tyne, UK
3. Royal United Hospitals Bath NHS Foundation Trust, Bath, UK
Corresponding author:
Mr Max Bitterlin
Vascular Science Unit, Bristol Royal Infirmary, University Hospitals Bristol and Weston NHS Foundation Trust, Marlborough Street, Bristol BS2 8HW, UK
Email: [email protected]


")

")

