ORIGINAL RESEARCH
A national UK-wide survey of tranexamic acid use in vascular surgery
Atha K,1 Shah A,2 Fabes J,3,4,5 Bera K6,7
Plain English Summary
Why we undertook the work: During vascular surgery (surgery on major blood vessels of the body), some patients can lose a large amount of blood. Tranexamic acid (sometimes called TXA) is a medicine that reduces breakdown of clots and can reduce bleeding. It is widely used in other situations such as trauma, childbirth and heart surgery where it has been shown to save lives and to reduce serious bleeding and the need for blood transfusions. However, TXA is not commonly used in vascular surgery. Vascular operations involve arteries, veins and sometimes artificial or vein grafts, and doctors worry that TXA might cause dangerous blood clots. These clots could block blood flow to important organs and limbs. At present there is not enough strong evidence to clearly show whether TXA is safe or helpful for patients having vascular surgery. We wanted to find out how TXA is currently used across the UK in vascular surgery, what doctors think about its risks and benefits, and whether there is support for more research.
What we did: We carried out a UK-wide survey of vascular surgeons and anaesthetists. Doctors were asked how often they use TXA in different planned (elective) and emergency vascular operations. They were also asked about their concerns regarding bleeding and blood clots, and whether they believed further research was needed. The survey included doctors from most vascular units across the UK, providing a national overview of current practice and opinions.
What we found: We found that TXA is rarely used in vascular surgery. Most doctors only give TXA when there is severe bleeding, rather than as a standard treatment. Doctors were especially concerned about blood clots during procedures where keeping arteries or grafts open is critical. TXA was therefore used very infrequently in operations such as carotid artery surgery and leg bypass surgery, where even a small clot could have serious consequences. In emergency situations such as surgery for a ruptured abdominal aortic aneurysm, TXA was used more often, particularly when there was major blood loss. Even so, practice varied widely between hospitals and between doctors. Most doctors felt that the current evidence about TXA use in vascular surgery is not enough. Many said they would support and take part in a future research study provided patient safety – especially the risk of blood clots – was carefully assessed.
What this means: TXA use in vascular surgery varies widely across the UK and is usually limited to situations involving heavy bleeding. Doctors remain cautious because of concerns about blood clots affecting vital blood vessels or grafts. However, TXA may have important benefits for some patients, particularly in operations where the risk of blood loss and the need for blood transfusion is high. In these situations, TXA may reduce bleeding and transfusion requirements. There is strong support for further research, including a carefully designed clinical trial, to determine whether TXA can be used safely and effectively in vascular patients. Such research should focus not only on bleeding but also on important safety outcomes such as stroke, graft blockage and the need for further surgery.
Abstract
Background: Tranexamic acid (TXA) is widely used to reduce perioperative bleeding in several surgical specialties; however, its role in vascular surgery remains uncertain. Concerns regarding arterial, venous and graft thrombosis, together with limited and low-certainty evidence of efficacy, have contributed to variation in practice across the UK. According to the 2025 National Vascular Registry there were nearly 20,000 major vascular operations carried out across the four nations. The 2023 NHS Blood and Transplant audit found TXA uptake in vascular surgery to be low (26.5%) when compared with other specialties such as cardiac, orthopaedic and trauma surgery, which each had TXA use over 80%. We set out to understand clinician perspectives to inform the design and possible need for a future trial.
Methods: We conducted a national cross-sectional survey of vascular anaesthetists and surgeons across the UK between December 2024 and June 2025. The questionnaire assessed TXA use in elective and emergency vascular procedures, perceptions of bleeding and thrombotic risk, and views on the adequacy of existing evidence and the feasibility of a future randomised controlled trial (RCT). Quantitative data were analysed descriptively and free-text responses were analysed thematically.
Results: A total of 142 responses were received from 49/65 (74.6%) UK vascular units. This included 85 anaesthetists and 57 surgeons, the majority of whom were consultant grade. Routine TXA use was uncommon across elective procedures, while selective use increased in the context of major haemorrhage, particularly during emergency surgery. Respondents perceived carotid surgery and lower limb revascularisation as carrying the highest risk of arterial or graft thrombosis, whereas trauma and major lower limb amputation were viewed as highest risk for venous thromboembolism; these perceptions were reflected in reported practice. Support for further research was high: 67/85 anaesthetists (79%) and 36/57 surgeons (63%) believed that an RCT evaluating TXA in vascular surgery is needed, with most favouring inclusion of both elective and emergency procedures. Willingness to recruit patients was reported by 77/85 anaesthetists (90%) and 42/57 surgeons (74%), although respondents noted that recruitment would depend on procedure type and multidisciplinary agreement. Safety considerations dominated views on trial design. Graft or arterial thrombosis up to 90 days was prioritised by 83/85 anaesthetists (98%) and 53/57 surgeons (93%), followed by return to theatre for bleeding or thrombosis and transfusion requirements. Most respondents (74/85 anaesthetists (87%) and 45/57 surgeons (79%)) indicated they would change practice if a well-designed trial demonstrated both safety and efficacy.
Conclusion: TXA use in vascular surgery is variable and context dependent. There is substantial clinical equipoise and strong support for a randomised trial, providing the study design reflects procedural heterogeneity and prioritises safety-related outcomes.
Introduction
Tranexamic acid (TXA) is a synthetic lysine analogue that inhibits fibrinolysis and reduces surgical bleeding by stabilising clot formation.1 Large randomised trials have demonstrated its efficacy in a range of clinical settings including trauma, postpartum haemorrhage and cardiac surgery, where TXA has been associated with reductions in mortality, critical bleeding and transfusion requirements.2-5 National and international guidelines, including NICE guidance on blood transfusion, recommend TXA for all surgical patients with anticipated blood loss exceeding 500 mL, irrespective of surgical specialty. However, these recommendations are not specific to vascular surgery and do not address some of the specialty-specific concerns.6,7
In vascular surgery, TXA use has been less consistent,8 largely related to concerns around vessel and/or graft thrombosis.9,10 A recent systematic review and meta-analysis of randomised trials of TXA in vascular surgery found no evidence of increased arterial or venous thromboembolic events, and no clear reduction in critical bleeding or transfusion requirements.11 However, the certainty of the evidence was low due to small sample sizes, few events and heterogeneity in study design, patient selection, dosing regimens and outcome reporting. As a result, whether TXA is beneficial, safe or indicated in vascular surgery remains uncertain.
The 2025 National Vascular Registry (NVR) report showed that there were 6,982 lower limb revascularisations, around 2,500 elective abdominal aneurysm repairs, nearly 6,000 carotid endarterectomies and over 3,800 major lower limb amputations carried out. National audit data in the UK consistently show a low rate of TXA administration in patients undergoing vascular surgery (26.5%) and who are potentially eligible to receive TXA compared with other specialities such as orthopaedics (92.7%).12 Surveys from other health systems have indicated wide variation in TXA use in vascular surgery and differences in practice and opinions between anaesthetists and surgeons.13 Whether similar patterns exist in the UK is unknown.
The feasibility of conducting a vascular-specific randomised controlled trial (RCT) of TXA in the UK, including willingness to recruit, appropriate endpoints and concerns regarding safety, has not been systematically evaluated. We therefore conducted a national survey to: (1) assess vascular surgeons’ and anaesthetists’ perceived risk of thrombosis and bleeding and understanding of the available evidence; (2) ascertain current patterns of TXA administration in vascular surgery; and (3) obtain views to inform the design of a future TXA RCT in vascular surgery.
Methods
This report has been prepared according to the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) guideline14 (see Appendix 1 online at www.jvsgbi.com).
A national cross-sectional survey was conducted between December 2024 and June 2025. A questionnaire was piloted internally and the survey wording was shared with and approved by the research committees of the Vascular Anaesthesia Society of Great Britain and Ireland (VASGBI) and Vascular Societies of Great Britain and Ireland (VSGBI) prior to circulation. The survey was hosted on the VASGBI online survey platform. Members of VSGBI and VASGBI were invited to participate through direct email communication and professional mailing lists; no financial incentives were provided. Several answers per unit were allowed. An example template of the survey is provided in Appendix 2 online at www.jvsgbi.com.
The survey was developed iteratively by a multidisciplinary team comprising vascular anaesthetists and surgeons. Questions evaluated current patterns of TXA use in elective and emergency vascular procedures, risk–benefit perceptions, beliefs regarding the need for further research and willingness to enrol patients in a future RCT. Both closed-response questions and free-text fields were included. Free-text fields were optional, but all other questions were mandatory resulting in no missing responses or incomplete forms. Closed-response questions used categorical frequency scales (eg, ‘routinely’, ‘used only in major haemorrhage’, ‘rarely’, ‘never’), and respondents were asked to select procedure-specific responses for elective endovascular abdominal aneurysm repair (EVAR), open abdominal aortic aneurysm (AAA) repair, lower limb revascularisation, major lower limb amputation, carotid endarterectomy and ruptured AAA (open and endovascular). Items relating to potential trial recruitment, outcome prioritisation and TXA dosing were also included.
Data were analysed descriptively. Categorical responses were summarised as frequencies and proportions. Free-text responses were grouped into broad thematic categories which emerged during analysis using a descriptive non-formal thematic approach. The map was created using Datawrapper, and Graph Pad Prism 10 was used to create all other figures.
Results
Respondents
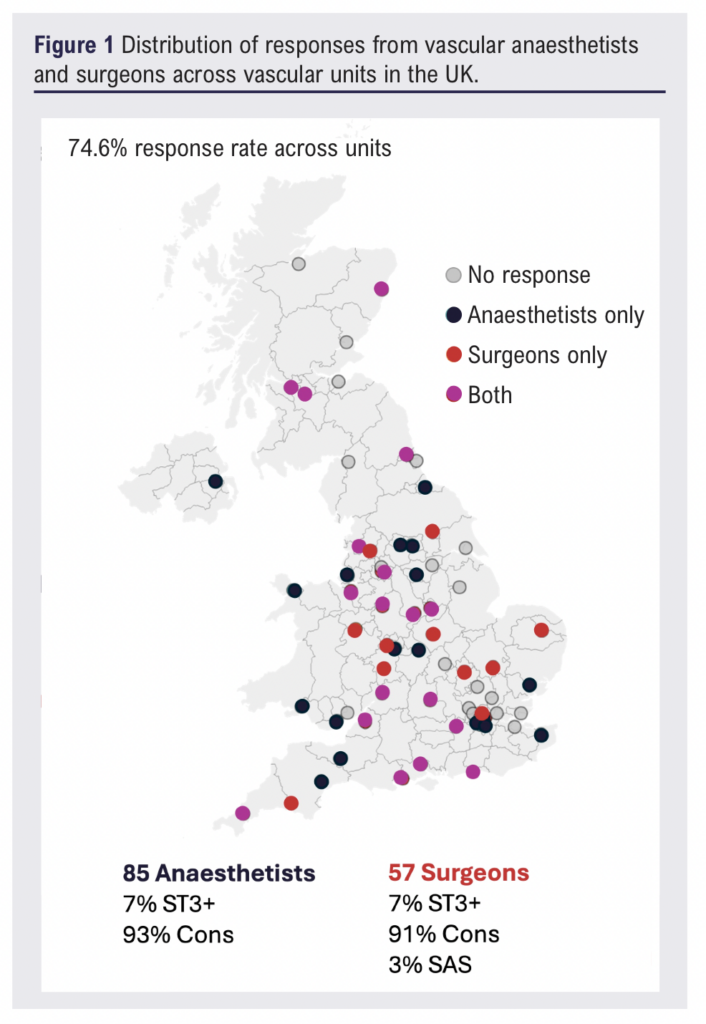
A total of 142 survey responses were received from 49/65 (74.6%) UK vascular units. Of these, 85 respondents were anaesthetists and 57 were surgeons. The majority of respondents (~90%) were consultant grade, with a small proportion in training (7% at ST3+). Responses were received from institutions across the UK, indicating broad national coverage (Figure 1).
Perceived risk of thrombosis and bleeding
Respondents were asked to rank the perceived risk of venous thromboembolism (VTE) and arterial or graft thrombosis across seven common vascular procedures. Trauma and major lower limb amputation were identified as having the highest VTE risk (78% and 73%, respectively) by both surgeons and anaesthetists. In contrast, lower limb revascularisation was viewed as the procedure with the highest risk of arterial or graft thrombosis, selected by 44/57 (77%) surgeons and 72/85 (85%) anaesthetists, followed by carotid endarterectomy and stenting (selected by 37/57 (64.9%) surgeons and 42/85 (49.4%) anaesthetists). This perception was echoed in free-text responses, with respondents frequently expressing concern about graft occlusion. For example, one surgeon noted “clot is your enemy” and questioned the rationale for TXA use when anticipated blood loss is minimal but thrombotic risk is substantial.
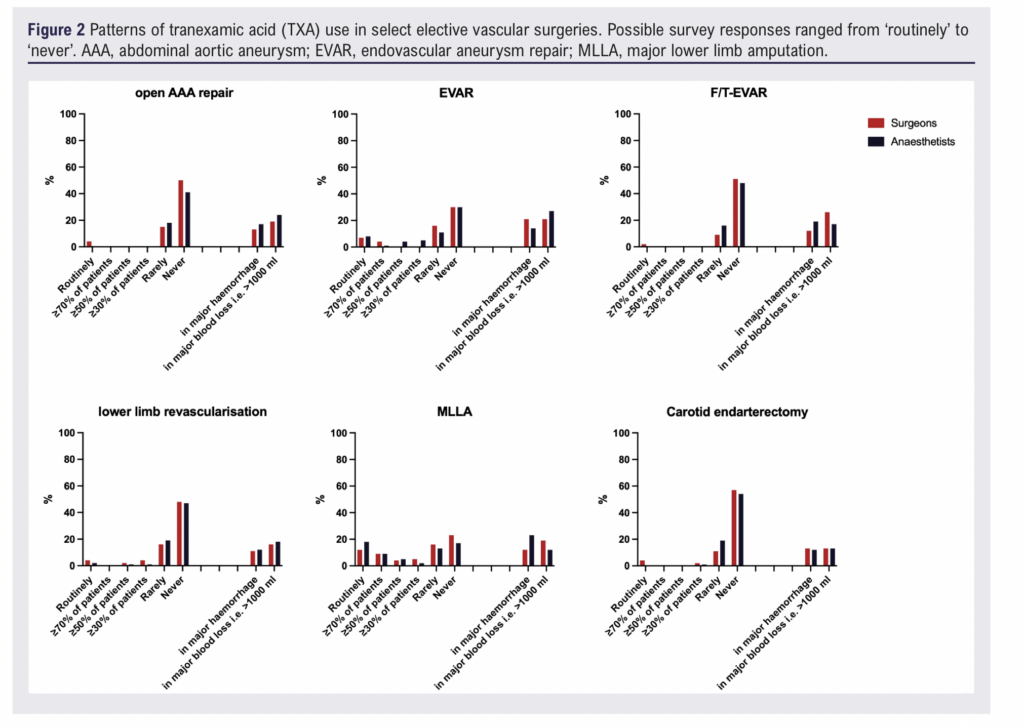
Current practice in elective surgery
Across all elective procedures, TXA use was infrequent. For elective EVAR, open AAA repair, lower limb revascularisation and major lower limb amputation, most respondents indicated that TXA was ‘rarely’ or ‘never’ used. Fewer than 10% of respondents reported routine administration in any elective procedure.
There was, however, a consistent increase in administration in the context of major haemorrhage. For elective AAA surgery, 12/57 (21%) surgeons and 22/85 (27%) anaesthetists reported giving TXA when blood loss exceeded 1000 mL. Practice for lower limb revascularisation and amputation followed similar patterns, although the absolute proportion of routine or selective use remained low (Figure 2).
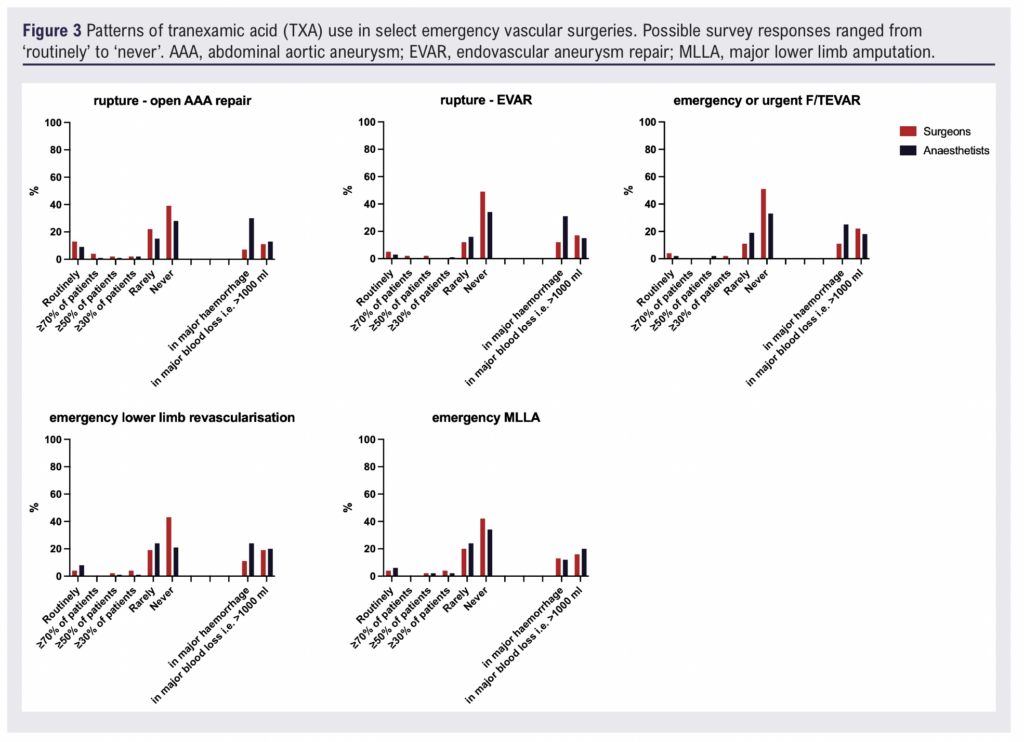
Current practice in emergency surgery
Greater variability was observed in emergency practice. For ruptured AAA, 18% of anaesthetists (15/85) reported routine use of TXA during open repair compared with 12% of surgeons (7/57). Routine use was less common for ruptured EVAR. As with elective procedures, the use of TXA increased during major haemorrhage, with several respondents indicating administration when blood loss was >1000 mL, regardless of procedure type (open repair vs EVAR).
For emergency lower limb revascularisation and amputation as well as emergency carotid surgery, TXA was rarely used routinely, although a minority of clinicians administered TXA selectively in cases of major bleeding (Figure 3).
Directions for future research
The majority of respondents expressed support for further research evaluating the role of TXA in vascular surgery. Overall, 67/85 (79%) anaesthetists and 36/57 (63%) surgeons believed that an RCT was needed, with most favouring a study including both elective and emergency procedures. There was broad consensus that the current evidence is insufficient to guide practice in this specialty, particularly given the perceived heterogeneity of risk across vascular procedures (Figure 4).
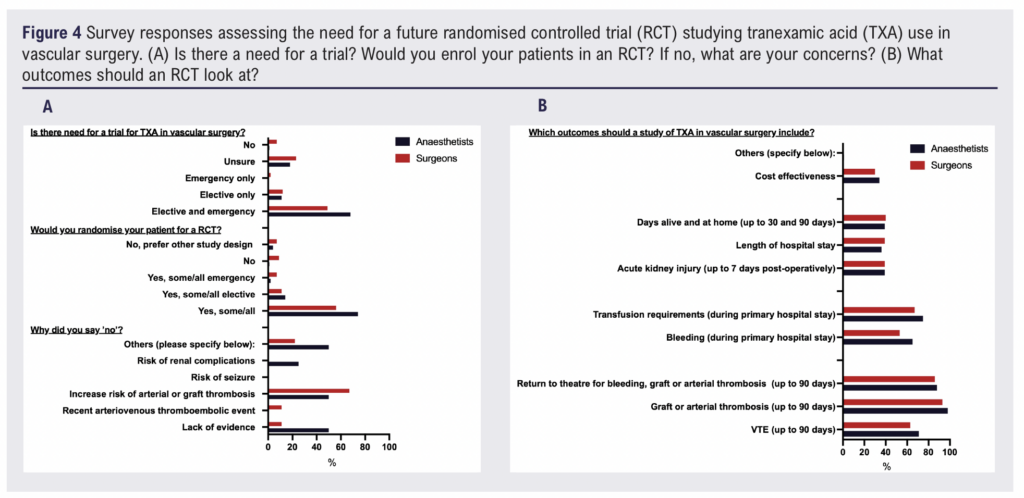
In addition to recognising the need for further evidence, most clinicians indicated that they would be willing to participate in an RCT (77/85 (90%) anaesthetists and 42/57 (74%) surgeons). The most common position was that participants would consider randomising some or all potential patients, with the extent of willingness varying according to procedure type. Several respondents noted that successful enrolment would depend on multidisciplinary agreement between surgeons and anaesthetists (Figure 4).
Although only a minority of respondents reported that they would not enter any patients into a trial (four anaesthetists and nine surgeons), those with reservations raised consistent concerns. The most cited concern was the perceived risk of arterial or graft thrombosis (two anaesthetists and six surgeons), particularly in operations in which patency is essential to limb perfusion or stroke prevention (Figure 4).
Respondents were also asked to identify outcomes that they considered important for any future study. The most selected outcomes were graft or arterial thrombosis up to 90 days (83/85 (98%) anaesthetists and 53/57 (93%) surgeons), return to theatre for bleeding or thrombosis (75/85 (88%) anaesthetists and 49/57 (86%) surgeons), and transfusion requirements (64/85 (75%) anaesthetists and 38/57 (67%) surgeons. Perioperative VTE was also frequently selected. Other outcomes including acute kidney injury, length of stay, days alive and at home, and cost-effectiveness were chosen less frequently. These results indicate that safety-related endpoints were prioritised more often than measures of clinical efficacy (Figure 4).
Lastly, respondents were asked whether they would change their practice if a study showed that TXA was both safe and effective; 74/85 (87%) anaesthetists and 45/57 (79%) surgeons indicated that they would alter practice in accordance with results from a well-designed and effectively conducted trial.
Preferred dosage of TXA
Most respondents indicated that they would use a 2 g dose, consistent with current national recommendations (53/85 (62%) anaesthetists and 35/57 (61%) surgeons).15 A smaller proportion favoured a 1 g dose (22/85 (26%) anaesthetists and 11/57 (19%) surgeons) and very few stated that they would not use TXA at all. Free-text comments highlighted uncertainty regarding the optimal dose, timing relative to heparinisation and the need for evidence specific to vascular patients.
Qualitative analysis
The optional free-text responses provided some important and interesting additional insights complementing the survey responses and reflected both recognition of uncertainty and support for further high-quality evidence. The two emerging themes of the free-text comments were identified as: (1) need for further evidence with demonstration of superiority; and (2) importance of multidisciplinary agreement and collaboration. One anaesthetist commented: “I am so glad you are asking this question”, while another emphasised the central concern underpinning current practice, stating: “I need strong evidence that it is harmless and makes the outcome significantly better before I start using it in vascular cases”. Similarly, surgeons expressed reservations about routine use in the absence of robust data, with one noting: “I just don’t feel there is enough evidence to justify its use in this patient cohort”. There were expressed safety concerns, with one surgeon noting: “The paper you quote specifically excluded vascular patients. I just don’t feel there is enough evidence to justify its use in this patient cohort. I can’t remember a death from bleeding, but I remember plenty related to ischaemic events: stroke, ischaemic bowel, MI, etc”. Two participants described prior adverse experiences or institutional anecdotes, including cases of limb loss following what they believed to be inappropriate TXA administration in the context of ruptured AAA. Other respondents questioned whether an RCT was feasible in a population with multiple confounding variables including comorbidities, antiplatelet or anticoagulant use, variations in surgical technique and the timing of TXA administration relative to intraoperative heparinisation. One respondent reflected this concern, stating: “There are so many variables that contribute to bleeding, which include the continued use of antiplatelets (mono and dual antiplatelet therapy), timing of heparinisation and, most importantly in my view, the surgical technique”. A small number (one anaesthetist and two surgeons) suggested that the existing evidence base was sufficient or that alternative designs, such as observational data or pooled registry analyses, might better address remaining uncertainties.
Discussion
In this national survey of vascular surgeons and anaesthetists we found that TXA use in vascular surgery was infrequent, with routine administration uncommon across both elective and emergency procedures. When used, TXA was most frequently given in the context of major haemorrhage and rarely in procedures associated with minimal blood loss. Despite national recommendations supporting TXA for surgical bleeding, respondents reported considerable variation in practice, reflecting specialty-specific concerns and differences in perceived risk. Additionally, while large contemporary trials such as POISE-3 included patients undergoing non-cardiac surgery including vascular procedures, procedural subtypes were not reported in detail and distinctions between elective and emergency vascular operations were not specified. Given the heterogeneity in bleeding and thrombotic risk across vascular operations, extrapolation to specific vascular contexts remains challenging, which may partly explain the ongoing variation identified in our survey.
A key finding was the contrast between perceived bleeding and thrombosis risks across procedures. Respondents consistently identified carotid surgery and lower limb revascularisation as operations with a high risk of graft or arterial thrombosis, whereas trauma and major lower limb amputation were viewed as highest risk for VTE. These differences are likely to influence decision-making; procedures with limited expected blood loss and high thrombosis risk were associated with low levels of TXA administration whereas TXA use was more common in operations with major haemorrhage, particularly ruptured AAA repair. This procedural variation illustrates that clinicians appear to consider TXA within the context of specific operative risks rather than applying uniform practice. However, volume of anticipated blood loss alone may not fully capture bleeding-related risk. In anatomically constrained procedures such as carotid surgery, even limited haemorrhage may have clinically relevant consequences, suggesting that the relevance of TXA may depend not only on the volume of bleeding but also on the potential impact of bleeding in specific operative contexts. Although there appeared to be differences in use rate between anaesthetists and surgeons (with higher reported use rate by anaesthetists), this might reflect responses from different units where different practice might have been agreed; this should not be interpreted as different practice between specialties.
Most respondents supported further research, with the majority of anaesthetists and surgeons indicating that an RCT was needed. These findings suggest that equipoise exists, yet practical considerations (eg, dose and timing of TXA, nature of procedure) may be essential for recruitment.
Respondents prioritised safety-related outcomes specific to vascular surgery for any future RCT. Graft or arterial thrombosis up to 90 days, return to theatre for bleeding or thrombosis, and transfusion requirements were the most frequently selected endpoints. Measures of bleeding alone were selected less often, indicating that clinicians were more concerned with avoiding thrombotic complications than reducing modest blood loss. These preferences have implications for trial design; outcomes should focus on both bleeding and thrombosis, and follow-up should extend beyond the immediate perioperative period to capture clinically relevant events such as graft failure and stroke.
This survey highlights the need for procedure-specific and context-specific evidence. Vascular surgery encompasses a heterogeneous group of operations that vary widely in expected blood loss, duration and risk of thrombosis. Elective procedures such as carotid endarterectomy, which typically involve minimal bleeding and are highly dependent on preserving arterial patency, may not warrant prophylactic TXA administration whereas open aortic surgery or ruptured aneurysm repair may represent circumstances in which TXA could be beneficial. Nonetheless, these scenarios also represent the settings in which the balance between bleeding control and arterial thrombosis is most precarious, as rupture complicated by acute limb ischemia is associated with high morbidity and mortality. Similarly, the distinction between elective and emergency surgery is relevant; TXA may be used more readily in emergencies with established or anticipated haemorrhage whereas its role in elective settings is less clear. Future studies should account for these differences rather than treating ‘vascular surgery’ as a uniform category.
It is noteworthy that national NHS Blood and Transplant (NHSBT) audit data report TXA administration in 26.5% of eligible vascular surgical cases, a figure higher than the rates of routine use reported in our survey (generally <10% in elective settings and up to 18% in emergency open repair). While these findings do not directly align, several factors may explain the disparity. First, our survey captured self-reported routine practice, which may further reflect clinicians’ cautious approach to prophylactic use. Second, the NHSBT data do not specify procedural context (eg, elective versus emergency surgery or specific operation types). In our study TXA use was higher in emergency ruptured aneurysm repair, suggesting that aggregate audit figures may reflect case mix rather than uniform practice across procedures.
Limitations
This study has certain limitations. Firstly, it relied on self-reported practice, which may not reflect actual use in theatre, and the number of respondents from some units was small. We disseminated our survey widely to vascular surgeons and anaesthetists, but acknowledge that the response rate with 57 surgeons and 85 anaesthetists is low in the context of over 500 consultant vascular surgeons and nearly 500 consultant anaesthetists who are VASGBI members. However, we feel that receiving a response from almost three-quarters of all vascular units provides a good representation of current practice across the UK. Additionally, survey response bias is possible, although the high unit response rate and predominance of consultant grade participants suggest that the findings are reflective of current national practice. Moreover, we did not collect or analyse linked responses between surgeons and anaesthetists within the same unit (or perform unit level clustering analysis) and responses were anonymised at the individual level. As such, we were unable to determine whether reported differences reflected true intra-team variation or differences between institutions. Nevertheless, the survey provides the first national overview of TXA use in UK vascular surgery and identifies key priorities for research. The findings demonstrate support for an RCT, highlight the importance of multidisciplinary collaboration, and underscore the need to evaluate outcomes that reflect both bleeding and thrombosis risk.
Conclusion
TXA use in vascular surgery is inconsistent, and most clinicians reserve it for situations of major haemorrhage rather than routine administration. Respondents expressed broad support for further research, with willingness to recruit patients to a randomised trial providing the study design addresses safety concerns and reflects procedural variation. Outcomes relating to graft or arterial thrombosis, return to theatre and transfusion were prioritised, indicating that safety parameters are central to clinical decision-making.
These findings indicate that equipoise exists for a randomised trial of TXA in vascular surgery. Future research should focus on procedure-specific and elective versus emergency contexts, with attention to multidisciplinary agreement and clinically meaningful endpoints. Results from such studies are likely to inform best practice and guide the appropriate use of TXA in this diverse surgical population.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2026;5(2):77-84
Publication date:
February 27, 2026
Author Affiliations:
1. Research Fellow, Memorial Sloan Kettering Cancer Center, New York, USA
2. Consultant Anaesthetist, Imperial College Healthcare NHS Trust, London, UK
3. Consultant Anaesthetist, University Hospitals Plymouth NHS Trust, Plymouth, UK
4. Faculty of Health, University of Plymouth, UK
5. NIHR Southampton Biomedical Research Centre, UK
6. Senior Clinical Fellow, Department of Vascular Surgery, Oxford University Hospitals NHS Foundation Trust, Oxford, UK
7. Nuffield Department of Surgical Sciences, University of Oxford, Oxford, UK
Corresponding author:
Dr Kasia D Bera Nuffield Department of Surgical Sciences, University of Oxford, Oxford, OX3 9DU, UK
Email: Katarzyna.bera@ nds.ox.ac.uk


")

")

