CLINICAL AUDIT
An audit of Global Vascular Guidelines implementation at two large teaching hospitals in differing healthcare settings
Vijayanathan A,1 Bilyy A,3 Barki D,3 Patel A,2,3 Arudchelvam J,4,5 Sandford B3
Plain English Summary
Why we undertook the work: Chronic limb-threatening ischaemia (CLTI) is a serious illness where blood flow to the legs is very poor. This can cause pain, wounds that don’t heal, and even lead to leg amputation. In 2019, experts made a set of guidelines called the Global Vascular Guidelines to help doctors treat CLTI better. We wanted to see if hospitals are following these guidelines.
What we did: We looked at the care given to patients with CLTI over one month in two big hospitals—one in London, UK and one in Colombo, Sri Lanka. We checked if doctors followed the guidelines, including how they checked patients’ feet, if they used scoring tools, and if they did scans to look at blood flow.
What we found: Both hospitals did well with scans to check blood flow. But foot checks were often not done properly, especially for patients staying in hospital. Most doctors also did not use the scoring tools to tell how bad the illness was. The London hospital followed the guidelines better in its foot clinic, likely because trained podiatrists (foot experts) were involved.
What this means: Even well-equipped hospitals can find it hard to follow all the guidelines. Simple steps like training junior doctors, using checklists and having the right tools (like monofilaments for foot tests) could help; however, this is beyond the scope of this audit. Hospitals everywhere need support to follow these guidelines better and improve care for people with CLTI.
Abstract
Objective: The Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia provide a framework for assessment and management of patients with chronic limb-threatening ischaemia (CLTI). This audit describes compliance with Global Vascular Guidelines (GVG) standards across two teaching hospitals in different healthcare settings.
Design: This is a prospective, cross-sectional, clinical audit conducted over a 1-month period.
Methods: All new CLTI patients admitted or seen in the outpatient podiatry clinic at Guy’s and St Thomas’ Hospital (GSTT) and the National Hospital of Sri Lanka (NHSL) between 1 May 2024 and 31 May 2024 were included. Data were collected regarding clinical assessment, scoring system and imaging utilisation according to recommendations set out in the GVG. Statistical significance was analysed with Fisher’s exact test using SPSS.
Results: 65 inpatients were included (GSTT: 38; NHSL: 27) and 49 outpatients (GSTT: 21; NHSL: 28). Among the inpatients, GVG-compliant medical history was recorded in 57 (88%) cases (GSTT: 32 (84%); NHSL: 25 (93%), p=0.311). GVG-compliant foot examination was completed in 10 (15%) patients (GSTT: 10 (26%); NHSL: 0 (0%), p=0.004). Use of non-invasive imaging was consistent between groups. Among the outpatients, GVG-compliant foot examinations were performed in all 21 outpatients at GSTT (100%) but in none of the 28 outpatients at NHSL (0%, p<0.001). Limb severity scoring systems were used for all outpatients seen at GSTT (21/21, 100%), whereas only 5 of 28 outpatients at NHSL (18%) had scoring systems documented (p<0.001). Non-invasive imaging utilisation was comparable between the two institutions for outpatients.
Conclusions: Implementation of the GVG is challenging, with even large teaching hospital centres failing to meet all the recommendations for assessment of patients with CLTI. Commonly missing parameters relate to examination and scoring systems. Further work is needed to understand the barriers to implementation and address these. This was a single cycle audit and further work has not been conducted to recycle this audit.
Introduction
Chronic limb-threatening ischaemia (CLTI) is the most severe form of peripheral arterial disease, associated with high rates of morbidity, mortality, and limb loss.1 CLTI creates significant costs to healthcare systems across the globe. Between 2020 and 2021 alone, the financial burden of non-elective amputations cost the National Health Service (NHS) over £115 million.2 Therefore, minimising these risks and resource utilisation is highly desirable. The Global Vascular Guidelines (GVG) were published in 2019 and provide a comprehensive evidence-based framework for the assessment and management of CLTI to improve patient outcomes.3 Effective implementation of clinical guidelines raises the standard of care, reduces expenses as well as inconsistent practices and decreases the risk of avoidable errors and adverse events.4 Additionally, guideline-based care has been shown to improve patient outcomes across various medical specialties.5-9
Currently, literature evaluating the global rates of compliance with GVG is scarce. In a single-centre study in Japan, patients with CLTI who received distal bypass revascularisation in line with GVG recommendations showed satisfactory outcomes in terms of limb salvage, graft patency, wound healing and survival. These results support the real-world effectiveness of GVG bypass recommendations as an initial revascularisation strategy.10 However, guideline adherence can be challenging due to variations in healthcare infrastructure, resources, variations in clinician practice and availability of locally designed guidelines.11 As a result, many low- and middle-income countries depend on guidelines developed in high-income settings despite lacking the multidisciplinary teams and specialist equipment required for effective implementation.12,13 Based on this context, the authors propose that implementing the GVG in non-high-income countries may be particularly challenging due to resource limitations. To date, no studies have evaluated compliance of healthcare institutions with GVG best practices.
This study audits compliance with GVG recommendations across two large teaching hospitals in contrasting healthcare settings: Guy’s and St Thomas’ Hospital (GSTT) in London and the National Hospital of Sri Lanka (NHSL) in Colombo. By assessing differences and similarities, this audit aims to identify areas for improvement and strategies to enhance guideline implementation globally.
Methods
Study design and setting
A single-cycle, prospective, cross-sectional, clinical audit was conducted over a one-month period from 1 May to 31 May 2024 at two large teaching hospitals: GSTT in London and NHSL in Colombo, Sri Lanka.
Participants
The audit included all acutely admitted inpatients with a diagnosis of CLTI or those managed on an outpatient basis in podiatry clinics at both institutions during the study period. No formal sample size calculation was undertaken as this was an observational audit of routine clinical practice over a defined period. As this was a prospective audit including all eligible patients within the study period, no formal power calculation was performed. As per the GVG, the diagnosis of CLTI was defined as a clinical syndrome characterised by the presence of peripheral arterial disease in conjunction with rest pain, gangrene or lower limb ulceration of more than 2 weeks’ duration.3
Ethics and approvals
The audit received a GSTT service-level approval (audit number: 15955) and underwent local organisational audit approval at NHSL. All data collection was based solely on the documentation in the patient record systems.
Data collection procedures
A proforma was designed to ensure uniform record keeping across both institutions (Figure 1). All inpatient data were collected from the initial admission clerking note in compliance with institutional protocols for maintaining patient confidentiality.

Assessors
In Sri Lanka, all assessments were performed by vascular surgeons ranging from registrars to consultants. In the UK, inpatient and outpatient assessments were conducted by vascular surgery consultants and middle-grade doctors, with specialist podiatry staff leading outpatient foot assessments. Equipment provided in GSTT included handheld Doppler machines on specialist vascular wards in the inpatient setting and ankle-brachial pressure index (ABPI) and toe-brachial pressure index (TBPI) equipment in the outpatient setting along with monofilament probes in both settings. This equipment was not always available in outlying wards or the Emergency Department. At NHSL this included access to Doppler machines in the inpatient setting but limited specialist equipment in the outpatient setting, with no access to ABPI or TBPI equipment or monofilaments and limited access to Doppler machines.
Variables and outcome measures
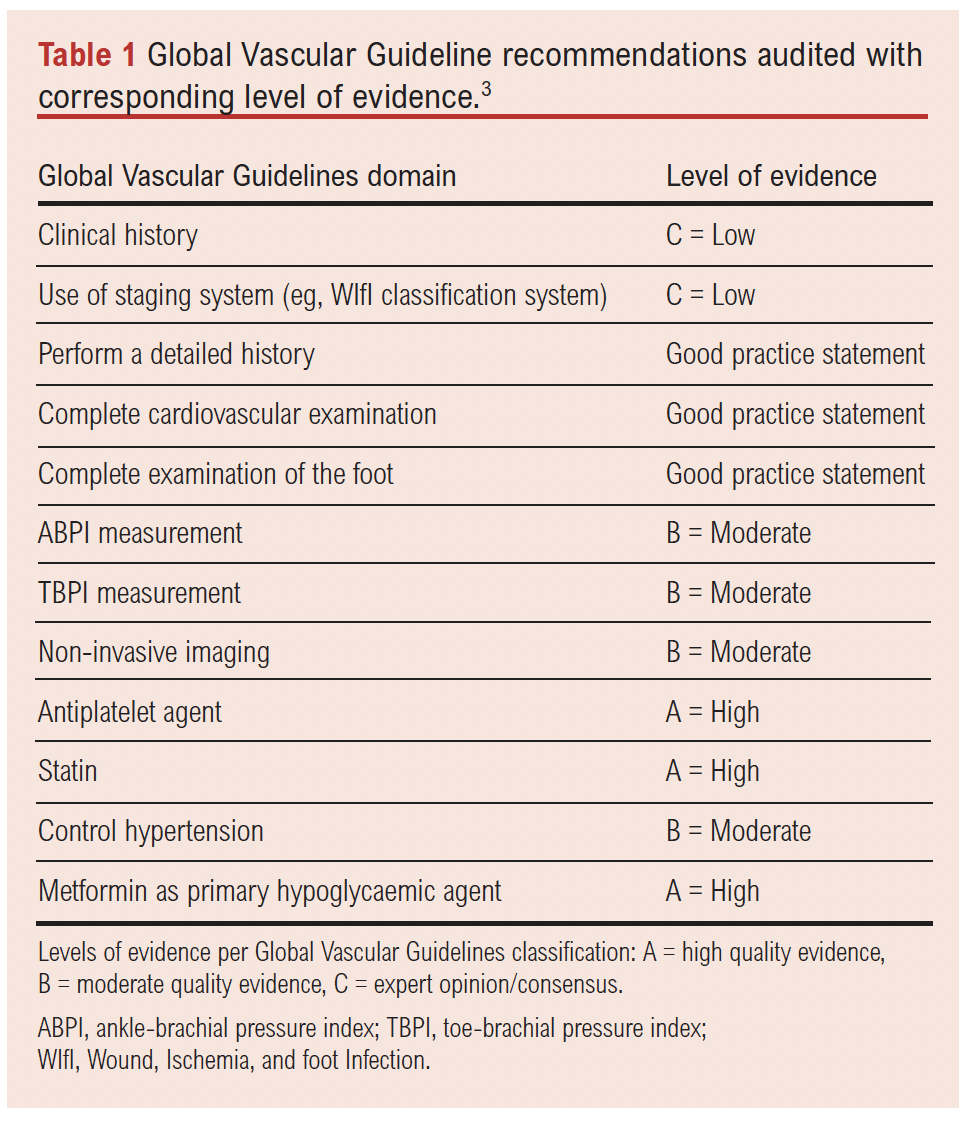
The audit assessed compliance with key recommendations across multiple GVG domains, including diagnosis and limb staging. For clarity and to facilitate interpretation of compliance, the exact GVG recommendations audited, along with their corresponding level of evidence, are summarised in Table 1. Levels of evidence were extracted directly from the GVG, where ‘A’ denotes high-quality evidence, ‘B’ moderate, ‘C’ low, and ‘good practice statement’ reflects expert consensus without formal grading.
Data collection focused on clinical assessment, scoring systems and non-invasive imaging use. First, the documentation of medical history was reviewed to confirm whether presenting symptoms (eg, rest pain and tissue loss), past medical history (such as diabetes, hypertension and renal disease) and atherosclerosis risk factors (including smoking and hyperlipidaemia) were recorded. For detailed history and foot assessment, the documentation was considered compliant only if all parameters listed in the proforma were documented (as per best medical practice recommendations of the GVG). Second, foot examination practices were audited to assess the documentation of pedal pulses, neuropathy testing and ulcer probing (where applicable) to evaluate depth, infection or exposure of underlying structures. Third, the use of limb severity scoring systems, such as the Wound, Ischemia, and foot Infection (WIfI) classification, was examined to determine their role in disease severity assessment and management decisions. Finally, compliance with recommendations for non-invasive imaging including duplex ultrasonography and computed tomography (CT) angiography was evaluated to assess vascular disease extent.
Data sources and management
Demographic data including patient age and sex were recorded. At GSTT, data were extracted from electronic medical records while, at NHSL, patient records were reviewed from paper-based documentation. All data were collected by trained clinicians familiar with the audit framework. To ensure reliability, 10% of the patient records were randomly selected for cross-checking by a second reviewer.
Missing data
Missing data were documented as ‘not recorded’ and excluded from percentage compliance calculations for that specific parameter, but included in denominators for overall compliance where appropriate. This was handled by one of the doctors overseeing this project.
Statistical analysis
Data were analysed using SPSS statistical software. Categorical variables were summarised as frequencies and compared between GSTT and NHSL using the two-tailed Fisher’s exact test, as several variables had small cell counts that did not meet the assumptions for the χ² test. The Fisher’s exact test was applied to all categorical comparisons to ensure consistency across analyses. Continuous variables such as patient age were reported as medians with interquartile ranges (IQR). Statistical significance was set at p<0.05.
Results
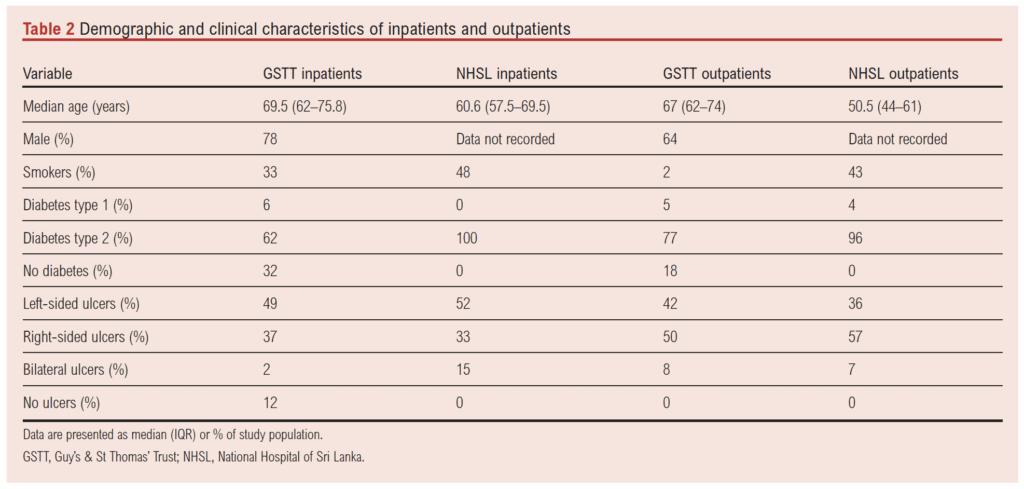
A total of 65 inpatients (GSTT: 38; NHSL: 27) and 49 outpatients (GSTT: 21; NHSL: 28) were included in this audit. Median ages for inpatients were 7.5 years older at GSTT than at NHSL, while outpatient median ages were 16.5 years older at GSTT than NHSL (see Table 2).
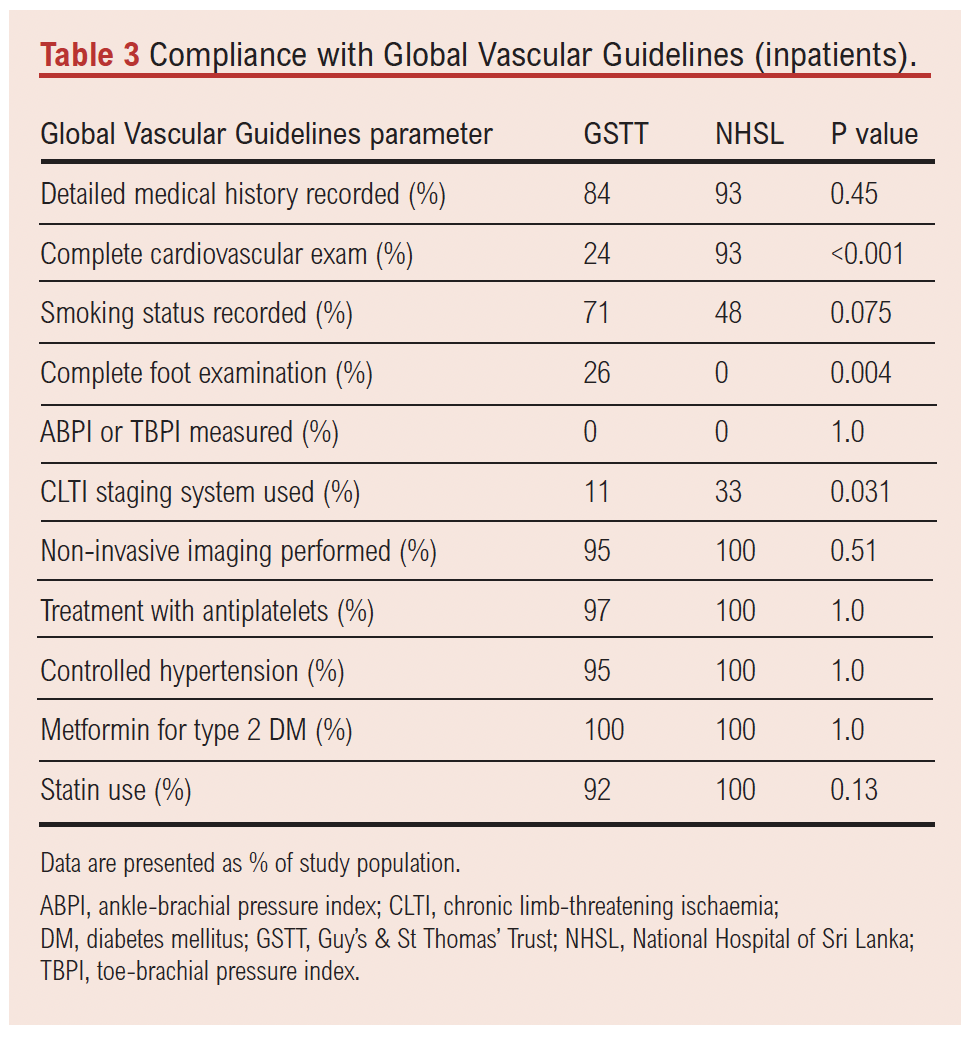
For inpatients, GVG-compliant medical histories including symptoms, past medical history and risk factors were recorded for the vast majority of patients. The compliance rates were similar between GSTT and NHSL.
GVG-compliant foot examination including pedal pulse assessment, neuropathy testing and probing of ulcers were poorly completed for inpatients at both GSTT and NHSL. Despite this, there was still a significant disparity observed between the two institutions, with no patients at NHSL having these investigations. At GSTT, the commonly missed parameters were neuropathy assessment (documented in 11 patients) and ulcer probing (documented in 10 cases). Whilst GVG-compliant foot examination was poorly performed at both centres, documentation of pedal pulses alone was significantly higher at NHSL than at GSTT, whereby all inpatients at NHSL had pedal pulses assessed. GSTT performed complete cardiovascular examinations considerably less often for inpatients than NHSL.
The use of limb severity scoring systems such as WIfI classification was low across both institutions, although significantly lower in GSTT than NHSL. Non-invasive imaging, including duplex ultrasound or other vascular imaging modalities, was consistently high at both hospitals. All NHSL patients received duplex ultrasonography as the modality of choice (see Table 3).
Among the 49 outpatients, significant differences in adherence to GVG recommendations were also observed (see Table 4). GVG-compliant foot examinations including documentation of pedal pulses, neuropathy assessment and ulcer probing were performed in all GSTT outpatients but in none of the outpatients at NHSL. Significant differences were also observed in performance of complete cardiovascular examination in the outpatient setting whereby no GSTT outpatients had this performed; this was only performed in the minority of NHSL outpatients.
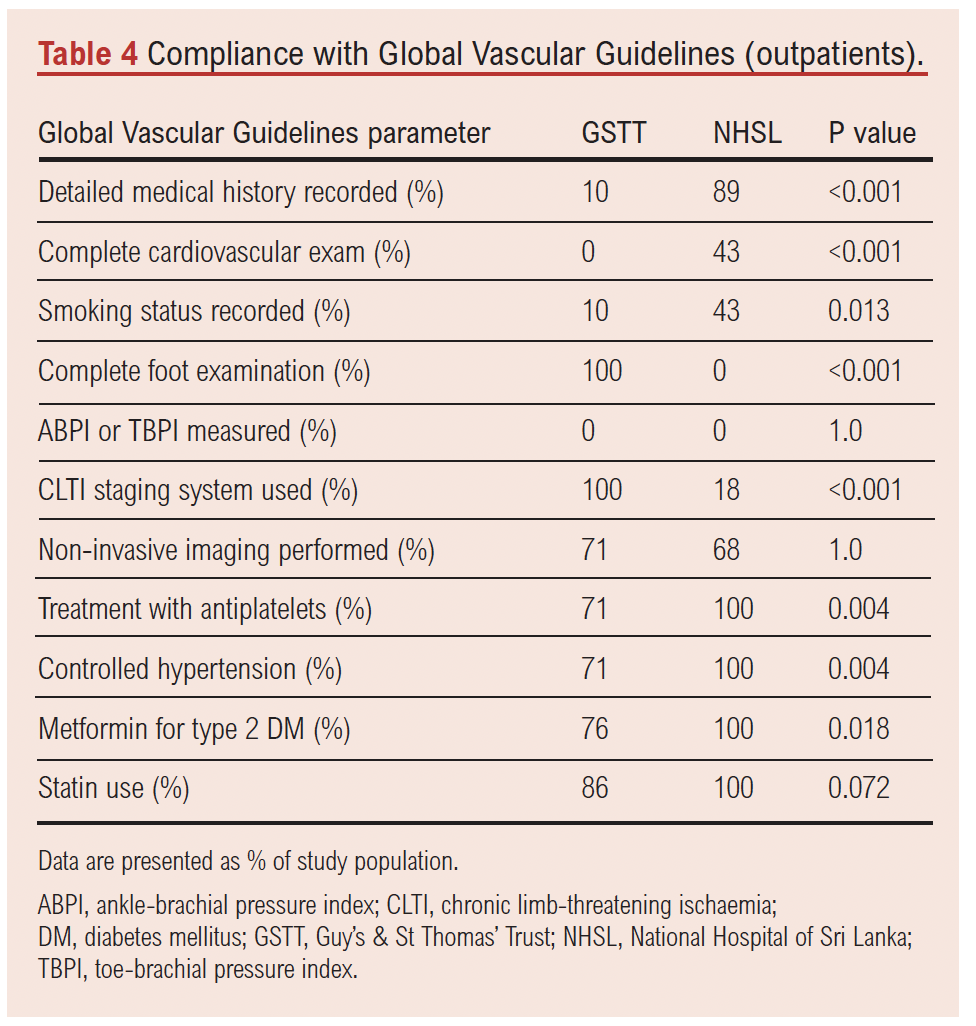
Limb severity scoring systems were used for all outpatients seen at GSTT whereas only a small minority at NHSL had scoring systems documented. The scoring system preferentially used in the GSTT outpatient setting was the Site, Ischaemia, Neuropathy, Bacterial infection, and Depth (SINBAD) classification.
Non-invasive imaging utilisation was comparable between the two institutions for outpatients; however, both were considerably less common than their inpatient counterparts.
Consistently, across inpatient and outpatient groups, NHSL pharmacologically reduced modifiable risk factors in all patients through the prescription of antihypertensives, statins and diabetes medication. This was also successfully performed for the majority of inpatients at GSTT, but considerably less in the outpatient setting.
In the inpatient setting, overall compliance with GVG was comparable but equally suboptimal (GSTT 63.2%; NHSL 69.8%). In the outpatient setting, the findings were similar (GSTT 54.1%; NHSL 60.1%).
Discussion
Various challenges in global implementation of clinical practice guidelines have been highlighted in the literature. Key obstacles include technological and attitudinal barriers, time constraints and lack of motivation, scepticism about validity and applicability, differences in professional practices, resource shortages and inconsistencies in staff training, all of which hinder widespread adoption and adherence to these guidelines.14-18
Challenges specific to vascular surgery have also been discussed in the literature. The lack of training in specialised techniques such as endovascular surgery are a key barrier to implementing vascular clinical guidelines in low- and middle-income countries.19 The limited availability of reputable training fellowships intensifies competition between newly qualified vascular surgeons and experienced practitioners already established in the field; however, these obstacles, although very relevant, were not applicable to the implementation of the assessment element of the guidelines.19 The impact of vascular disease is further exacerbated by the unavailability of essential surgical equipment combined with restricted access to surgeons.20,21
This audit highlights significant challenges in the implementation of the GVG at two major teaching hospitals operating in contrasting healthcare settings: GSTT in London and NHSL in Colombo. Despite the vast differences in their healthcare environments, neither institution demonstrated full compliance with GVG standards, underscoring universal barriers to their implementation.
A notable observation was the poor adherence to guideline-directed foot examinations, particularly among inpatients at both institutions. At NHSL in particular, despite consistent documentation of pedal pulses, crucial elements such as neuropathy assessments and ulcer probing were omitted across both inpatient and outpatient settings. It is possible that providing simple and cost-effective tools like monofilaments and ulcer probes in the inpatient setting could improve disease severity assessment and support clinical decision-making; however, specific auditing of availability of equipment was not carried out as this was beyond the scope of this audit. In contrast, GSTT excelled in outpatient foot evaluations, achieving 100% compliance in that parameter. The success of this service may be linked to the specialised expertise of the podiatry team leading it, rather than rotational medical staff who face challenges in maintaining protocolised institutional care due to the need for ongoing training.22 Additionally, the use of a standardised proforma for outpatient pedal assessments – a method known to improve documentation consistency and enhance patient outcomes – likely contributed to its effectiveness.23 The disparity between the hospitals could stem from differences in healthcare infrastructure (ie, availability of an electronic patient record system at GSTT providing ease of documentation), training and resources (lack of monofilaments compromises complete clinical evaluation of neuropathy), but this is beyond the scope of this study to further investigate. Although consultant-led ward rounds at GSTT emphasised pedal pulse assessments, initial patient evaluations on admission were often conducted by junior residents. There could be several barriers to complete examination by junior residents such as lack of confidence in their foot examination skills due to inadequate training or failure to complete assessments because of competing clinical demands or practical barriers faced during overnight admissions such as removal and re-application of dressings. Data were not collected in this study to identify the root causes for a lack of compliance. At NHSL clinicians appeared to depend more on thorough clinical examination and pedal pulse assessment compared with GSTT.
Another striking finding was the minimal use of the WIfI limb severity scoring system at both institutions. This system is integral to the GVG framework, providing a structured approach to stratifying disease severity and estimating the risk of major limb amputation, need of revascularisation and even time to wound healing.3 Despite its importance, both institutions failed to meet this GVG recommendation. The ‘ischaemia’ component of the WIfI score is determined using haemodynamic measurements including the ABPI or TBPI.24 However, neither hospital demonstrated use of the necessary equipment to conduct these assessments in the inpatient setting, highlighting that resource limitations can persist even in high-income healthcare systems. Interestingly, despite its availability in the outpatient setting in GSTT, the guidance for ABPI and TBPI was poorly adhered to, suggesting that access to equipment may not be the most important factor driving its use. Addressing this gap in guideline implementation would require not only the provision of appropriate diagnostic tools but also structured clinician training and institutional backing to ensure integration into routine practice.15,20
Notably, GSTT achieved full compliance in using a scoring system within the outpatient podiatry service. However, their chosen system was the SINBAD classification – the most commonly used diabetic foot ulcer tool in the UK – known for its simplicity as it requires no specialised equipment.25 Despite its widespread use, the WIfI classification offers superior outcomes compared to SINBAD, including more accurate predictions of one-year amputation risk and ulcer healing times. Consequently, broader adoption of the WIfI system could lead to improved patient outcomes and informed shared decision-making in both high- and low-to-middle-income healthcare settings.25
Non-invasive imaging, a cornerstone of CLTI assessment, was one area where both hospitals demonstrated high compliance. Nearly all GSTT inpatients (except for those deemed for palliation, n=2) and all NHSL inpatients underwent non-invasive imaging studies, reflecting the prioritisation of diagnostic vascular assessment in both settings. The parity in imaging utilisation suggests that this aspect of the GVG may be more feasible to implement universally, even in resource-constrained environments like NHSL. Of note, in the absence of contraindications, the routine non-invasive imaging modality at NHSL was duplex ultrasonography whereas the GSTT patient cohort tended to undergo CT angiography as the investigation of choice. Identification of vascular anatomy through imaging is crucial for planning revascularisation strategies. While duplex ultrasonography remains a valuable diagnostic tool, its limitations have been highlighted in previous studies.26 Conversely, CT angiography is often favoured for surgical planning due to its ease of use and the comprehensive anatomical detail provided by cross-sectional imaging, but it may not be readily available in a low-income setting due to increased financial costs.27
Another challenge of translating comprehensive guidelines like the GVG into real-world practice is the presence of national guidelines that may differ from those proposed globally. In the UK the management of CLTI follows the National Institute for Health and Care Excellence (NICE) guidelines which, while aligned with the GVG in many aspects, differ in certain domains.28 For example, the use of CLTI staging systems is not outlined in the guidance and therefore may not be included in routine clinical practice across the UK. However, given the well-documented prognostic value of the WIfI system, integrating this staging tool into routine care could offer long-term benefits in patient management.3,24,25
A further issue, particularly evident at NHSL, was physical access to a vascular surgeon. Due to limited resources, many CLTI patients were forced to travel for hours to attend their appointments and had to rely on relatives or public transportation. Although not directly measured in this audit, inability to access a vascular unit may cause diagnostic and treatment setbacks, causing substantial delays in revascularisation of CLTI patients. Risks of postoperative major amputations and in-hospital death are associated with delayed presentation and management.29 It has also been shown that a presentation delay of 2 weeks is an independent predictor of major limb amputations.30 Therefore, healthcare infrastructure remains a key component for best patient outcomes.
It is notable that several high-evidence recommendations such as antiplatelet therapy and statin use achieved high compliance in both settings, whereas lower-evidence or good practice recommendations such as detailed foot examination or staging system use showed marked variation. This pattern suggests that the strength of evidence underpinning a recommendation may influence its prioritisation in clinical practice, an observation consistent with previous literature on guideline adoption.
While the strengths of this study include the comprehensive quality of the data from two vascular units with tertiary referral practices and wide inpatient and outpatient coverage, it has several limitations. It is an audit based on figures over a short period of time. Additionally, it lacks follow-up data to assess one-year major limb amputation rates, mortality and time to healing of ulcers. Finally, it is unclear whether the observed low rates of compliance with the GVG recommendations affect patient outcomes.
Moving forward, tailored interventions are essential to improve GVG adherence. Both high-resource and resource-limited healthcare systems may benefit from simplified protocols that prioritise fundamental high-impact components of the guidelines. For instance, ensuring the availability of bedside equipment for comprehensive foot examinations (eg, monofilaments for neuropathy assessment, TBPI machines) and promoting the use of limb severity scoring tools could significantly enhance guideline adherence and long-term outcomes without requiring substantial resource investment. High-resource settings like GSTT must address documentation gaps, recognise the need for clinical training of junior residents and explore opportunities to integrate guideline components (ie, scoring systems) into standardised electronic health records and workflows.
Conclusion
The implementation of the GVG remains suboptimal in both resource-limited and resource-rich healthcare settings. While each setting presents unique barriers, common deficiencies – particularly in foot examination and scoring system utilisation – highlight the need for enhanced resources and education, streamlined workflows and context-specific adaptations of the guidelines. Addressing these challenges will be essential to improving CLTI outcomes globally and ensuring equitable access to evidence-based care.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2025;4(4):215-222
Publication date:
August 28, 2025
Author Affiliations:
1. Guy’s, King’s and St Thomas’ School of Medical Education, King’s College London, London, UK
2. School of Cardiovascular Medicine & Sciences, King’s College London, London, UK
3. Department of Vascular Surgery, Guy’s and St Thomas’ NHS Trust, London, UK
4. Department of Vascular Surgery, National Hospital of Sri Lanka, Colombo, Sri Lanka
5. Department of Vascular and Transplant Surgery, Faculty of Medicine, University of Colombo, Sri Lanka
Corresponding author:
Dr Anthony Vijayanathan
Guy’s, King’s and St Thomas’ School of Medical Education, King’s College London, London, UK
Email: [email protected]


")

")

