CASE REPORT
Surgical repair of a right proximal radial artery true aneurysm: case report and literature review
Chikhal R, Daysley H, Hemadneh M
Abstract
True radial artery aneurysms (RAAs) are exceptionally rare. We report a case of a 33-year-old man with an idiopathic fusiform true aneurysm of the proximal right radial artery, managed successfully via resection and reversed ipsilateral cephalic vein interposition bypass. Postoperative recovery was uneventful, with preserved distal perfusion and no complications at 6-month follow-up. This case underscores the importance of early surgical intervention for symptomatic RAAs and the efficacy of autologous vein grafts.
Introduction
Fewer than 24 true radial artery aneurysms (RAAs) have been reported since the first description by Thorrens et al in 1966.1 While most radial artery aneurysms are pseudoaneurysms secondary to trauma or iatrogenic injury,2 true aneurysms – characterised by dilation of all three arterial wall layers – are exceedingly rare, usually idiopathic but may be associated with connective tissue disorders.3 Their diagnosis requires a threshold dilation of 1.5 times the normal radial artery diameter (2–3 mm).3 This case underscores the diagnostic and surgical challenges of idiopathic RAAs, which lack established aetiological frameworks. Surgical repair is indicated for symptomatic aneurysms or those at risk of rupture/thromboembolism.2,4 We report a case of idiopathic true RAA treated with resection and vein graft reconstruction, highlighting diagnostic and technical considerations.
Case presentation
A 33-year-old man presented with a tender pulsatile mass in the right proximal forearm, present for 3 months, accompanied by an intermittent cold sensation in the index and middle fingers. Comprehensive history revealed no antecedent trauma, previous vascular procedures or systemic symptoms suggestive of connective tissue disorders. Comorbidities included hypertension (controlled with amlodipine and candesartan). There was no family history of connective tissue disorders or risk factors for peripheral arterial disease.
Examination revealed a mildly tender pulsatile mass over the proximal radial artery without thrill or bruit on auscultation. Allen’s test demonstrated an intact palmar arch. There were no signs of infection, thrombosis or distal ischaemia. A general examination was negative for pulsatile masses in the abdomen, groins or popliteal fossae. Neurological upper limb examination was normal.
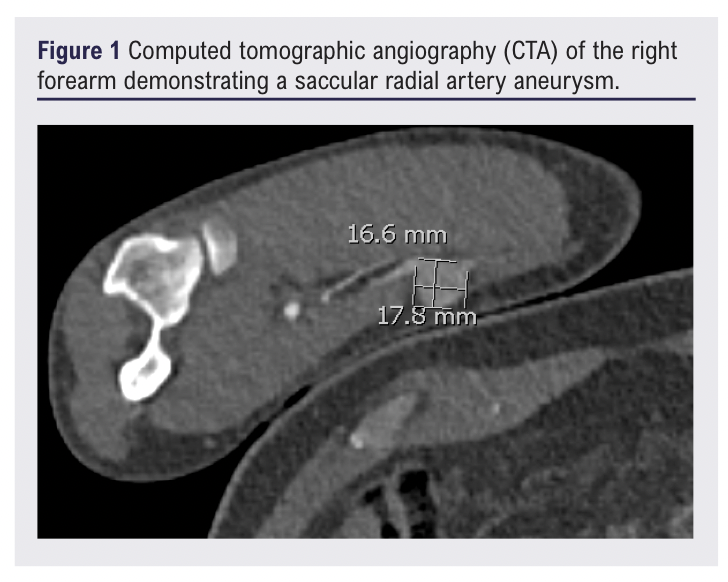
Laboratory studies showed no evidence of systemic inflammation, metabolic derangement or autoimmune pathology. Vascular imaging with duplex ultrasound and contrast-enhanced CT angiography identified a 16.6 × 17.8 mm wide-necked aneurysm originating 3 cm distal to the origin of the radial artery, with preserved patency of the distal radial and ulnar arteries (Figure 1). Incidental imaging findings included a bovine aortic arch variant, a common anatomical variation present in 15–35% of the population, with no evidence of atherosclerotic disease in the upper extremity vasculature.5
Full written informed consent from the patient was obtained for publishing this article and accompanying images.
Surgical management
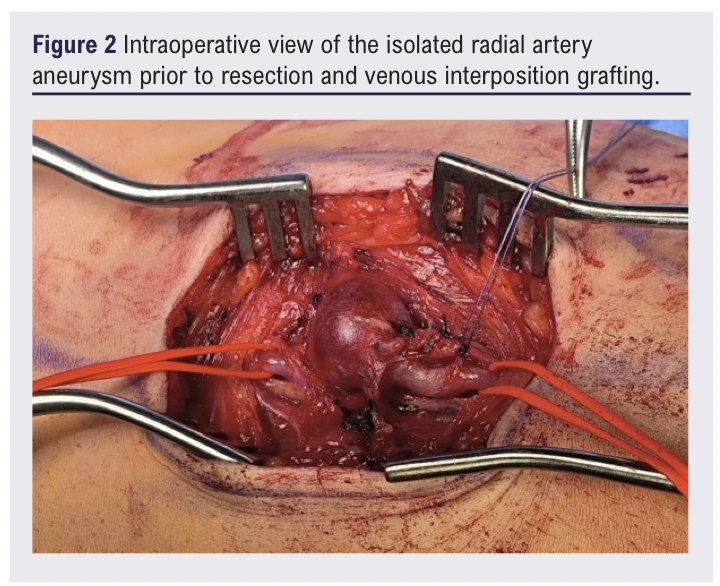
Due to the associated tenderness of the aneurysm and potential risks of complications (eg, distal thromboembolism, compression of neighbouring structures, and lifetime rupture risk), after discussion at the multidisciplinary team meeting and with the patient he was scheduled for surgical repair of the right proximal RAA.6 The surgical procedure was performed under general anaesthesia through a volar forearm approach. Meticulous dissection exposed the aneurysm while protecting the adjacent radial nerve (Figure 2). This incision was also used for the cephalic vein harvest which was later used for the bypass.
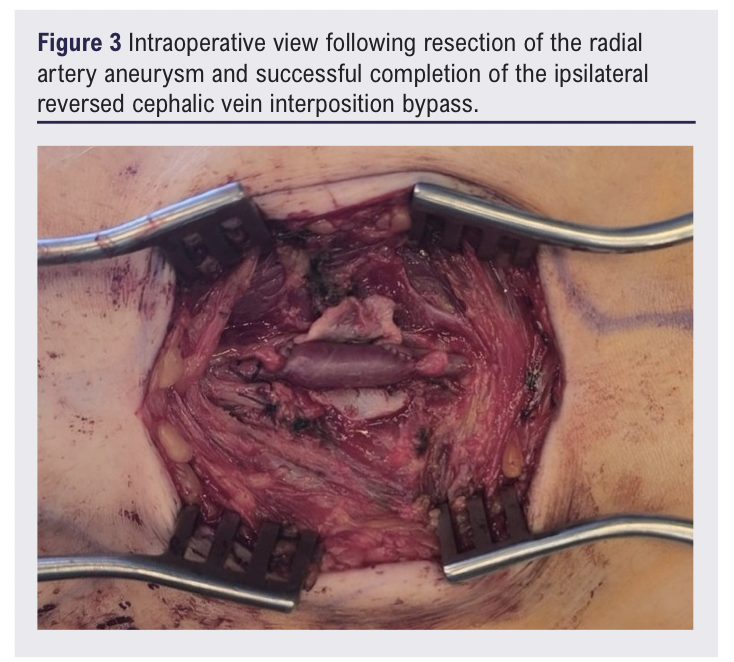
Proximal and distal control of the radial artery was achieved using bulldog clamps, and collaterals were controlled with 3/0 Vicryl slings. The aneurysmal segment was opened and arterial continuity was restored using an ipsilateral, reversed, short cephalic vein interposition bypass, anastomosed proximally and distally with 6/0 Prolene (Figure 3). Restoration of a palpable radial pulse confirmed graft patency and distal flow.
The decision to proceed with a cephalic venous interposition graft was made after considering several management options. Simple ligation of the radial artery was a feasible option, particularly given the patient’s patent ulnar artery and a negative Allen’s test confirming adequate collateral circulation. However, surgical revascularisation was selected to preserve a dual blood supply to the hand, an important consideration in a young patient. The cephalic vein was ultimately chosen as the conduit based on its optimal diameter match and the technical advantage of harvest without requiring an additional surgical incision.
Histopathological examination of the RAA wall confirmed the diagnosis of true aneurysm, demonstrating all three intact arterial wall layers with characteristic myxoid degeneration and fibrosis.
Outcome
The patient experienced an uncomplicated postoperative course and was discharged on the same day. At the 6-month follow-up appointment the patient was asymptomatic, with no sensory or motor deficits and a strong radial pulse and was subsequently discharged.
Discussion
This case of idiopathic true RAA contributes to the limited existing literature on this rare vascular condition. The clinical presentation – with a characteristic pulsatile mass and occasional distal coldness – aligns with previous case reports, although the absence of identifiable aetiology makes this case particularly noteworthy. The diagnostic approach, combining ultrasound and CT angiography, aligns with current best practices for vascular assessment.7 Autologous vein grafts remain a preferred choice for arterial reconstruction due to their high patency rates and durable adaptive remodelling under arterial haemodynamic conditions.8
A RAA is characterised by a localised dilation exceeding 1.5 times the normal diameter of the vessel, which typically measures 2–3 mm in healthy individuals.3 A true aneurysm involves all three layers of the arterial wall (intima, media and adventitia) and often results from structural weakening.3 While most RAAs are pseudoaneurysms caused by trauma or iatrogenic injury (eg, arterial cannulation), rare cases are associated with connective tissue disorders, repetitive occupational trauma or idiopathic aetiologies.9 RAAs typically present as a pulsatile mass and often require surgical intervention to mitigate potential complications including thromboembolic events or neurovascular compression.6,9 Clinical manifestations may include pain, sensory disturbances (such as numbness or paraesthesia) or signs of distal thromboembolism.4,9 While ultrasonography serves as the primary non-invasive diagnostic modality, advanced imaging techniques – including CT angiography, MR angiography and conventional angiography – provide comprehensive vascular assessment when indicated.10
The management of RAAs depends on the adequacy of the collateral circulation, assessed through diagnostic evaluations such as Allen’s test or Doppler ultrasound. When the collateral circulation is sufficient, simple ligation and resection may be performed without reconstruction as the ulnar artery can maintain adequate hand perfusion. In cases where reconstruction is necessary, particularly in patients with inadequate collateral flow or high functional demand, surgical options include interposition vein grafting, typically using the great saphenous vein or a cephalic vein graft. Alternatively, primary end-to-end anastomosis may be considered if tension-free repair is feasible. Endovascular techniques such as coil embolisation or stent grafting represent less invasive options for selected patients, although their long-term efficacy in RAAs requires further study. The choice of treatment is individualised, balancing anatomical considerations, patient factors and functional outcomes.
Conclusion
This case reinforces key principles in managing true RAAs. It underscores the necessity of definitive vascular imaging for diagnosis and planning, the importance of multidisciplinary team discussion to tailor management and the obligation of comprehensive patient consultation regarding the risks and benefits of intervention. Finally, it highlights that, even in apparently idiopathic cases, a thorough evaluation for occult systemic disorders is still an essential component of care.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2026;5(2):108-110
Publication date:
January 23, 2026
Author Affiliations:
Hull University Teaching
Hospital NHS Trust, Hull, UK
Corresponding author:
Dr Rohan Chikhal
Academic Vascular Surgical Unit
Hull University Teaching Hospital Trust, Anlaby Rd, Hull,
HU3 2JZ, UK
Email: [email protected]


")

")

