ORIGINAL RESEARCH
Development of a rehabilitation programme for individuals with chronic limb threatening ischaemia post revascularisation (HOPE): a modified Delphi study
Duff J,1 Saratzis A,2,3 Bartlett YK,4 Harwood AE,1 Haque A,4 Edwards H,1 Birkett S1
Plain English Summary
Why we undertook the work: Peripheral artery disease (PAD) is a condition that affects blood flow to the legs. Around 236 million people in the world have this condition and this number is likely to rise another 50% by 2045. Chronic limb threatening ischaemia (CLTI) is a serious form of PAD and often requires surgery to improve blood flow. After surgery, however, many individuals still experience poor mobility, pain and serious complications. Some of these complications can lead to amputation and many die within a few years. Rehabilitation is known to benefit people with other conditions, so the aim of this study was to design a rehabilitation programme specifically for individuals with CLTI after they have had surgery. In future we can then see if we can improve the outcomes of those with CLTI.
What we did: Patients, their carers and healthcare professionals took part in a three-round activity called a modified Delphi study. In the first step participants shared ideas about what should be included in a rehabilitation programme. In the second step they rated how important each idea was by either agreeing or disagreeing with them, or by prioritising them. If 70% or more people agreed that the idea was important it was included in the programme. In the final step participants discussed the ideas that had not achieved 70% and then re-voted. The ideas that achieved 70% or over were then added to the programme.
What we found: The group agreed on exercises that should be included in the rehabilitation programme, how often they should be done, where they should take place and how they should be monitored. The group also agreed on education topics that should be included in the programme and how they should be delivered.
What this means: Identifying key components is the first step in designing a rehabilitation programme for individuals with CLTI after they have had surgery. After finalising the programme, the next step is to see how useful and helpful it is in a real-life setting.
Abstract
Background: Peripheral artery disease (PAD) affects over 236 million people globally, with the prevalence continuing to rise. Its most severe form, chronic limb threatening ischaemia (CLTI), affects around 11% of PAD patients and carries high risks of amputation, cardiovascular events and mortality despite revascularisation intervention. Individuals with CLTI often experience poor mobility, frailty and reduced quality of life, yet no structured rehabilitation strategy exists following surgery. This study aimed to develop a novel rehabilitation programme for those with CLTI post revascularisation through a consensus-driven process involving patients, carers and healthcare professionals.
Methods: A multidisciplinary research team conducted a modified Delphi activity between November 2024 and June 2025. The team created the Round 1 questionnaires which were administered online and in paper format and distributed via social media and email networks. Open-ended questions pertaining to rehabilitation, exercise and education aimed to generate a comprehensive list of relevant items. In the Round 2 survey, participants evaluated the inclusion of these items in the rehabilitation programme by rating and prioritising them. Consensus was pre-defined as ≥70% agreement. The final round ran as an online workshop where all findings were presented to participants and items that had not achieved consensus were subjected to further review, discussion and re-evaluation through an online voting process.
Results: 57 participants completed the initial questionnaire. Of these, 20 were healthcare professionals and 37 were individuals with CLTI/carers. Content analysis of responses identified four key domains related to exercise (activities, frequency, location and monitoring) and three domains related to education (content, delivery method and timing). In Round 2, 29 participants responded (13 healthcare professionals and 16 individuals with CLTI/carers), and consensus was achieved on the exercise activities and educational content to be included in the rehabilitation programme. In the online workshop involving nine participants (six healthcare professionals and three individuals with CLTI/carers), consensus was reached on all remaining topics.
Conclusion: The findings informed the design of a novel individualised rehabilitation programme for individuals with CLTI following surgery. Future research is planned to assess the feasibility of this programme.
Introduction
Peripheral artery disease (PAD) affects over 236 million globally,1 equating to approximately 20% of individuals aged over 60 in the UK. Already identified as the leading contributor to vascular service demand within secondary care,2 the prevalence of this condition is projected to increase by 50% by the year 2045.3 The most severe manifestation of PAD is chronic limb threatening ischaemia (CLTI), characterised by rest pain and gangrene or ulceration lasting more than 2 weeks.4 Equating to around 11% of PAD cases,5 CLTI poses a significant threat to both limb viability and overall survival, necessitating prompt revascularisation either through open surgical or endovascular intervention to re-establish perfusion to the lower extremities.6
Despite undergoing revascularisation, patients with CLTI remain at considerable risk of adverse outcomes, especially amputation and cardiovascular events. Reported one-year and three-year mortality rates approach 50%, with major adverse cardiovascular events occurring in 42% of cases and amputation rates reaching up to 20% within the same time frames.6–8 Individuals affected by CLTI typically exhibit severely impaired ambulatory capacity, diminished physical fitness, a predominantly sedentary lifestyle, poor quality of life and clinical features of sarcopenia and frailty, all of which are independently associated with increased morbidity and mortality.9,10
In the absence of formal guidance such as a structured secondary prevention strategy following surgical intervention, these clinical trajectories are likely to deteriorate further. Consequently, there is an urgent need to develop and evaluate evidence-based rehabilitation protocols tailored to this high-risk population. While exercise therapy post-revascularisation has demonstrated efficacy in patients with intermittent claudication yielding significant improvements in walking distance and cost-effectiveness,11–14 its applicability to individuals with CLTI remains uncertain due to no existing evidence. Therefore, the aim of this project was to design a novel rehabilitation programme specifically for individuals with CLTI who have undergone revascularisation surgery. The objectives were to engage people with CLTI, their carers and healthcare professionals who have experience with CLTI in a Delphi exercise and to agree by consensus the structure, content and format of the programme.
Methods
Study design
A Delphi protocol was employed as this technique is widely adopted in health services research to harness the insights of healthcare professionals and individuals with lived experience of health conditions.15 In the absence of standardised methodology for Delphi studies,16 this study was characterised as a modified Delphi due to the use of a predefined framework that shaped the initial survey focusing specifically on rehabilitation, exercise and education topics, and the incorporation of an online consensus building workshop. The study was designed adhering to key principles17 and with an international multidisciplinary scope due to the lack of established CLTI-specific rehabilitation guidance globally.18
Based on the research aim, questions pertaining to rehabilitation, exercise and education questions were drafted (JD), refined (SB, YKB and AS) and reviewed (AEH, AH) for Round 1. The open-ended format allowed participants to provide a qualitative response anonymously.19 Two questionnaires (one for individuals with CLTI/carers and one for healthcare professionals) were created on Jisc Online Surveys,20 (a secure GDPR-compliant platform) and in paper-based format to enhance accessibility and participation. Pilot testing was conducted prior to dissemination.
The Round 1 survey included a participant information page and required consent to access the questions. A submit button on the final page permitted data collection. Participants could provide an email or postal address to receive the second survey and indicate consent to be contacted regarding the online workshop. The Round 2 survey employed both quantitative and qualitative formats to allow for rating, prioritising and free-text responses.21 Participants were asked to provide an email or postal address to be contacted regarding the Round 3 workshop and, in line with Round 1, a submit button on the final page permitted data collection. Round 3 employed an online workshop to facilitate qualitative discussion prior to a final anonymous online vote. This study was conducted and reported in accordance with Conducting and Reporting Delphi Studies (CREDES) guidance to enhance the transparency, methodological rigour and reproducibility of the findings.22
Steering group
A multidisciplinary team coordinated the study activity. The research team brings together expertise spanning health psychology, clinical exercise physiology, cardiovascular rehabilitation and vascular surgery, alongside individuals with lived experience. Collectively, the team has extensive experience in the co-design, delivery and evaluation of complex rehabilitation interventions using mixed-methods and consensus-based approaches, including Delphi studies that integrate patient and clinician perspectives.
Public and Patient Involvement and Engagement (PPIE)
As PPIE is paramount in shaping and powering healthcare research,23,24 it was embedded within this study. A recent James Lind Alliance (JLA) priority setting partnership identified the top 10 research priorities in PAD,25 which initiated the development of this research.26 A PPIE advisory group comprising five patients and carers with lived experience of CLTI reviewed the patient questionnaire and provided feedback. This informed several refinements prior to dissemination including rewording items, adding questions and including examples for clarity.
Participants
To optimise the qualitative strength of recommendations or consensus,27 individuals with CLTI, their carers and healthcare professionals were recruited. Our predefined criteria for participants were individuals living with CLTI, carers of individuals with CLTI and healthcare professionals with experience of CLTI such as vascular surgeons, vascular nurses, physiotherapists, podiatrists, occupational therapists and clinical exercise physiologists.
Sample size
While there is no universally prescribed sample size for Delphi studies,27 a range of 30–50 participants is generally considered optimal for studies involving homogenous groups.28 Given the modified nature of this Delphi protocol, a panel size of 30 was targeted, with emphasis placed on achieving balanced representation from both healthcare professionals and individuals affected by CLTI, including carers. No fixed upper limit was imposed; however, the research team agreed to close Round 1 should no novel concepts emerge, in accordance with established guidance.17
Recruitment
Two digital recruitment posters were created, one targeting individuals with CLTI/carers and the other healthcare professionals. These were disseminated via social media platforms including PAD support groups on Facebook and LinkedIn. Additionally, the research team used email networks and AS participated in a webinar hosted by an international PAD support group on Facebook to present the research project and encourage participation. Potential participants were able to access the initial questionnaire online via a QR code or hyperlink or, alternatively, to contact JD to request a paper copy.
Data collection and analysis
Data collection took place between November 2024 and June 2025. A three-round modified Delphi protocol was employed to elicit relevant topics, establish consensus and collaboratively inform the design of a rehabilitation programme.
Round 1
The first round (R1) comprised 13 open-ended questions that focused on rehabilitation, exercise and educational needs (see Appendix 1 online at www.jvsgbi.com). The open-ended structure and confidential nature of the questionnaires enabled respondents to elaborate freely, mitigating potential biases associated with group dynamics such as dominance and conformity.27 The survey opened on 15 November 2024 and the response rate was monitored by JD and SB who had access to the data. The survey closed on 5 February 2025 as the sample size had been achieved and no new data emerged. During this time frame no paper surveys were requested, completed or returned. The online data were exported onto an Excel sheet and analysed by JD who removed duplicates and categorised and sub-categorised free-text responses into relevant domains for the rehabilitation programme.29 These were subsequently discussed and finalised with the research team (JD, SB, AEH, YKB, AH and AS). This analysis informed the content and structure of the second round (R2) survey. Prior to sending out the R2 survey to participants, the content was checked against the original R1 responses by the research team (JD, SB, AEH, YKB, AH, AS) to ensure no relevant items were missing.
Round 2
The R2 survey comprised structured questions and statements, systematically developed from the domains identified in R1. Consistent with R1, the survey was available online and in paper-based format to ensure broad accessibility. Participants were asked to rate their agreement on the inclusion of elements of the rehabilitation programme via a Likert scale, with response options 1–3 from ‘agree’ to ‘disagree’. Where multiple options had been suggested in R1, all options were presented for prioritising – for example, participants were presented with a list of exercises and asked how often they should be performed. In this example response options were ‘1–3 times per week’, ‘4–6 times per week’ or ‘every day’.
The survey opened on 18 February 2025 and the response rate was monitored by JD and SB. In line with guidance,30,31 reminder emails were sent to non-responders on 7 March 2025 and 17 March 2025 and the survey closed on 29 March 2025 as no new data emerged. The analysis of R2 responses (JD) enabled the assessment of consensus (level of agreement) among participants.22 Given the variability in consensus thresholds across Delphi studies,22 a priori consensus was defined in this study as agreement equal to or exceeding 70%.
Round 3
Consenting participants were emailed the date and time of the workshop and a link to download Microsoft Teams32 on 16 May. Those who accepted were emailed a workshop agenda, the items to be discussed and a link to join the workshop.
The workshop took place on 27 June 2025 led by the research team with patients, carers and healthcare professionals in attendance. The aim was to confirm consensus from the previous round, explore and quantify levels of agreement on remaining items that had not achieved consensus, and finalise the elements to be included in the rehabilitation programme. At the start of the workshop, previous round results were presented (JD) highlighting items that had not achieved consensus. Participants were then split into two breakout rooms with members of the research team facilitating. The groups reconvened and key points were summarised by the research team. Participants then anonymously agreed or disagreed with seven statements on Jisc. The analysis of the R3 responses (JD) enabled the assessment of consensus (level of agreement) among participants. All items that achieved consensus in R1, R2 and R3 were used to inform the design of the rehabilitation programme.
Results
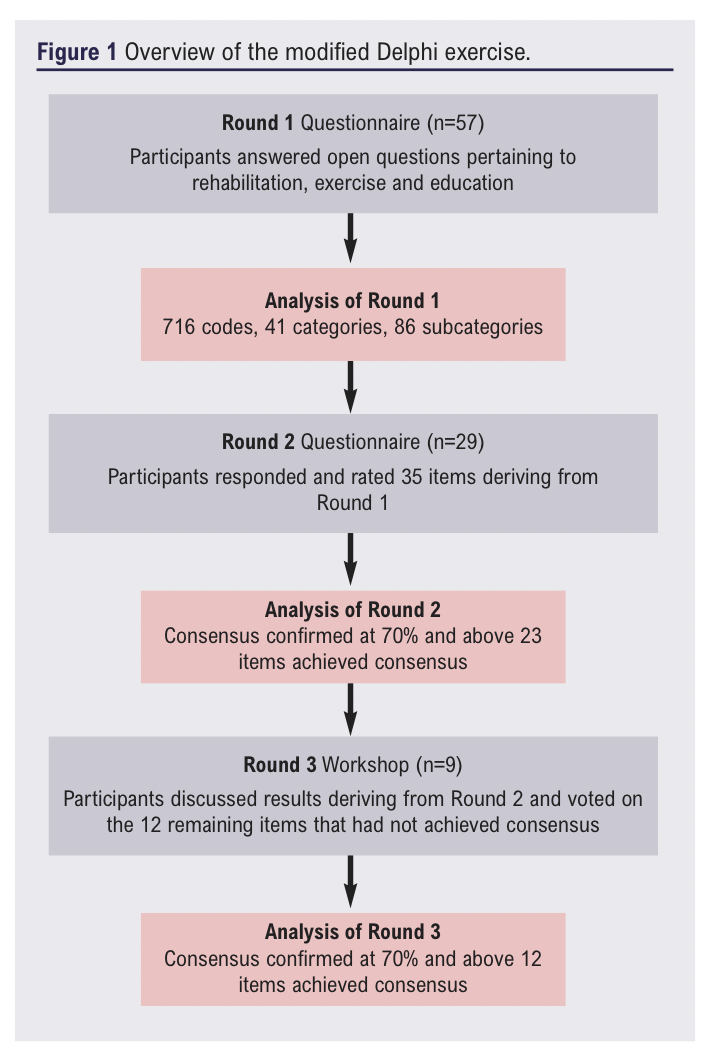
An overview of the modified Delphi exercise is shown in Figure 1.
Round 1: Open ended questionnaire
A total of 57 participants completed the initial questionnaire online; no paper surveys were requested. Participants comprised both healthcare professionals and individuals living with CLTI/carers (Table 1). Of these, 20 respondents were healthcare professionals, representing a multidisciplinary cohort that included vascular surgeons, radiologists, academic researchers, physiotherapists and podiatrists. All the healthcare professional participants were based in the UK, with geographical representation spanning diverse regions (both rural and urban) such as Liverpool, London, Birmingham, Leicester and Wales. Survey engagement was high, with a 100% response rate across all questions (20/20). Furthermore, all the healthcare professionals provided contact details for follow-up participation and 18 (90%) expressed an interest in attending the subsequent workshop.
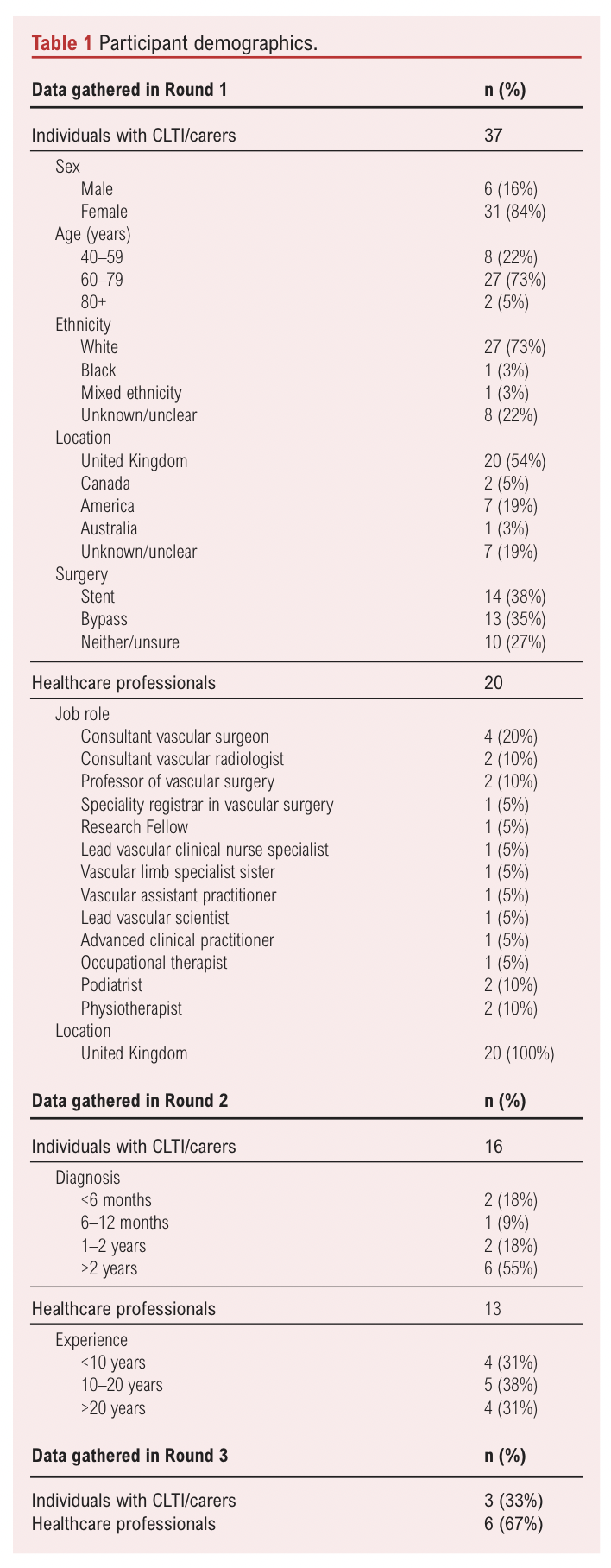
Of the 57 total survey respondents, 37 were individuals living with CLTI or carers of someone affected by the condition. Among this subgroup, 14 participants reported having undergone stent placement while 13 had received bypass surgery. Ten respondents either had not undergone surgical intervention or were uncertain about the procedure they had received. The cohort included 31 female and 6 male participants, with a mean age of 63±8.8 years. Geographical representation was broad, encompassing regions across England, Scotland, Wales, Canada, USA and Australia. Survey engagement was high with a response rate of 92% (34/37) across all questions. Additionally, 34 participants (92%) provided contact information for follow-up and 35 (95%) expressed interest in attending the subsequent workshop.
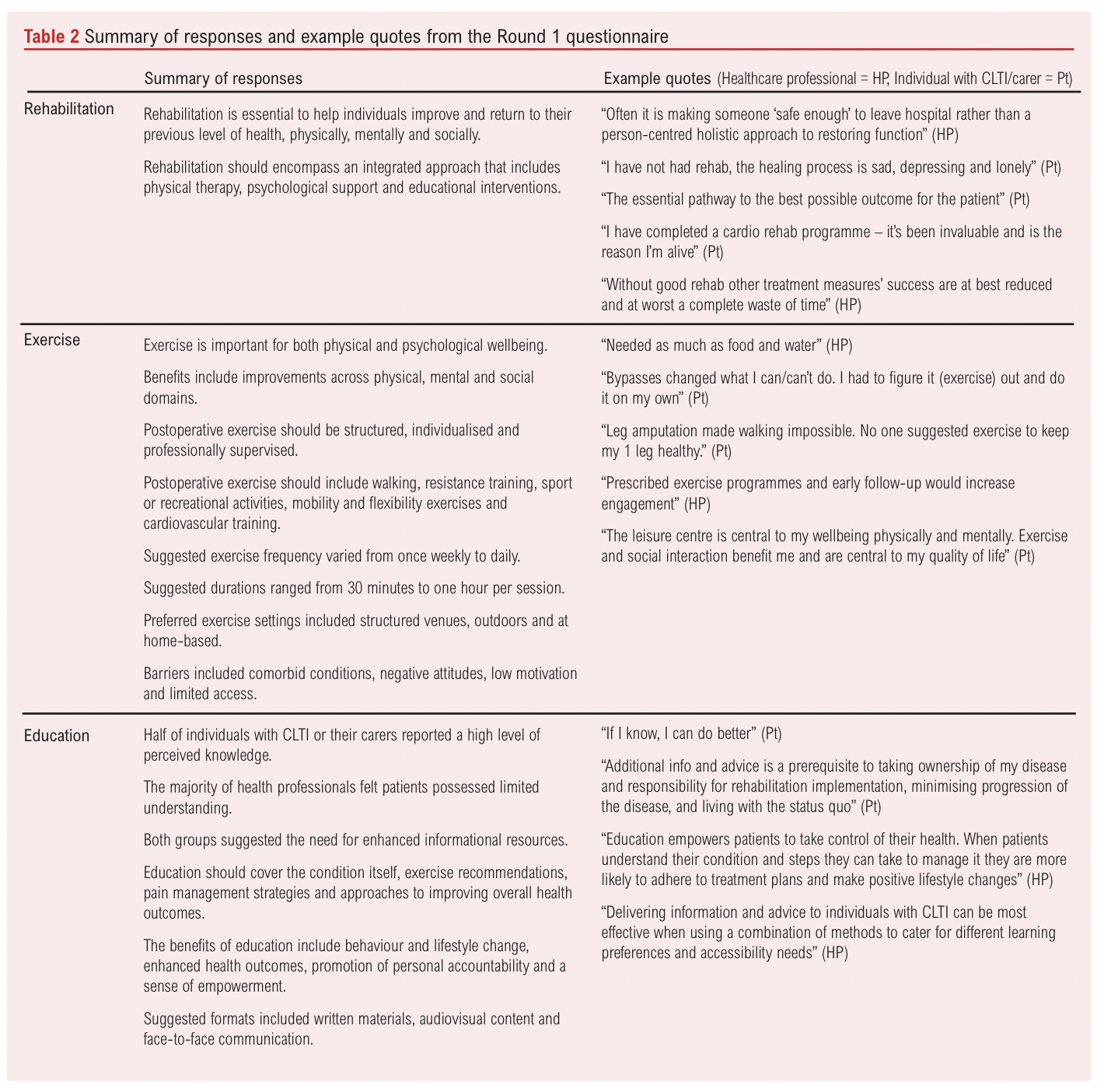
The R1 questionnaire responses yielded 716 individual codes after 236 duplicates had been removed. These were categorised and sub-categorised into domains. The domains were reviewed and refined by the research team (Table 2) and compared with the R1 responses. This resulted in 35 items presented for prioritisation or rating in the R2 survey, and a list of barriers to participation in rehabilitation which we aim to address when developing the programme content.
Round 2: Questionnaire to assess consensus
A total of 29 participants completed the R2 questionnaire. This cohort included 13 healthcare professionals, each with an average of 10–20 years of clinical experience in managing CLTI, and 16 individuals with lived experience of CLTI (either patients or carers). Among the latter group, the duration of diagnosis ranged from less than six months to over two years. Participants were asked to rate their agreement on the inclusion of certain elements in the rehabilitation programme or prioritise certain elements.
There was strong consensus (90%) that educational interventions would be beneficial for individuals with CLTI following revascularisation. Consensus was also reached on the inclusion of several key topics within the proposed education programme: the condition and what causes it (97%); other medical conditions and how they are related to CLTI (93%); outcomes and what happens if nothing is done (90%); types of surgery and what it achieves (83%); medication and pain management (86%); and management of risk factors (93%). No topics generated from R1 failed to achieve consensus. Eight additional topics were suggested in the free-text response. Of these, five did not generate any new themes (eg, prevention and walking with pain) and four were deemed out of scope (eg, when to get a second opinion and how to search for physicians).
Regarding delivery methods, person-led presentations were identified as the preferred format (74%), with consensus supporting the involvement of both healthcare professionals (97%) and individuals with lived experience of CLTI (76%) as facilitators. However, consensus was not reached on several aspects of programme design including the optimal duration of presentations (48% agreement for 10–20 minutes), the use of printed leaflets (56%), the inclusion of online video resources (67%) and the recommended length of such videos (52% agreement for 1–10 minutes).
There was strong consensus (90%) that exercise is beneficial for individuals with CLTI following revascularisation. Agreement was achieved on the inclusion of specific activities within the proposed exercise programme – namely, outdoor walking (93%), strength training (79%), balance exercises (83%), cardiovascular/aerobic activity (72%) and breathing or relaxation techniques (72%). Notably, all activities identified during R1 attained consensus for inclusion. Seven additional activities were suggested in the free-text responses. Of these, five had components comparable to current listed activities (eg, Nordic walking and yoga) and two were deemed out of scope due to accessibility and provision (eg, swimming).
Consensus was also reached regarding the recommended frequency of strength and cardiovascular exercises, with 79% and 70% agreement respectively that these should be undertaken 1–3 times per week. However, no clear consensus emerged on the optimal frequency for walking (48% agreement for 4–6 times per week), balance (50% agreement for 1–3 times per week) or breathing/relaxation exercises (59% agreement for every day).
In terms of preferred exercise settings, participants indicated that walking and breathing/relaxation activities are best conducted in the home environment (86% and 85%, respectively) whereas cardiovascular/aerobic sessions were considered more appropriate at a venue (81%). The optimal location for strength and balance exercises remained inconclusive. Additionally, 86% agreed that attending a supervised exercise session would provide social support, and the free-text responses identified additional provision of social support which we aim to address when developing the programme.
While 79% of respondents agreed that walking should be monitored using an activity tracker, consensus was not reached regarding appropriate methods for monitoring or recording strength training (36% agreement for a diary), balance (43% agreement for a diary), aerobic exercises (46% agreement for an activity tracker) and breathing/relaxation (50% agreement for a diary). In summary, of the 35 items presented for evaluation, 23 achieved consensus while 12 items did not meet this criterion.
Round 3: Workshop
A total of nine participants attended the final online workshop. Of these, six were healthcare professionals and three were individuals with CLTI/carers. Twelve items pertaining to exercise frequency, location, monitoring and educational delivery method and timings that had not achieved consensus in R2 were discussed in breakout rooms prior to voting taking place.
Consensus was achieved regarding the recommended structure and delivery of exercise and educational components for individuals with CLTI following revascularisation. It was unanimously agreed that walking should be undertaken 4–6 times per week (100%) and balance exercises should be performed 1–3 times per week (100%) at home (100%). There was consensus that breathing/relaxation activities should be practised daily (83%) also within the home setting (100%). Whilst there was agreement that strength training should be conducted in a designated venue (100%), there were also discussions during the workshop that strength training should also take place in the home. Furthermore, there was full agreement that all activities should be systematically monitored using a participant-maintained diary (100%).
In relation to educational delivery, consensus was reached that presentations should not exceed 20 minutes in duration (100%). Additionally, it was agreed that educational content should be made available in multiple formats, including printed leaflets (100%) and online videos (100%), with the latter recommended to have a maximum duration of 10 minutes (100%). Additional discussions during the workshop were that physical activity/exercise should be included as a stand-alone educational topic rather than embedded in the risk factors topic. In summary, all 12 items presented in the workshop achieved consensus.
Discussion
The primary aim of this study was to employ a modified Delphi to identify the key components to be included in an individualised rehabilitation programme specifically for individuals with CLTI following revascularisation surgery.
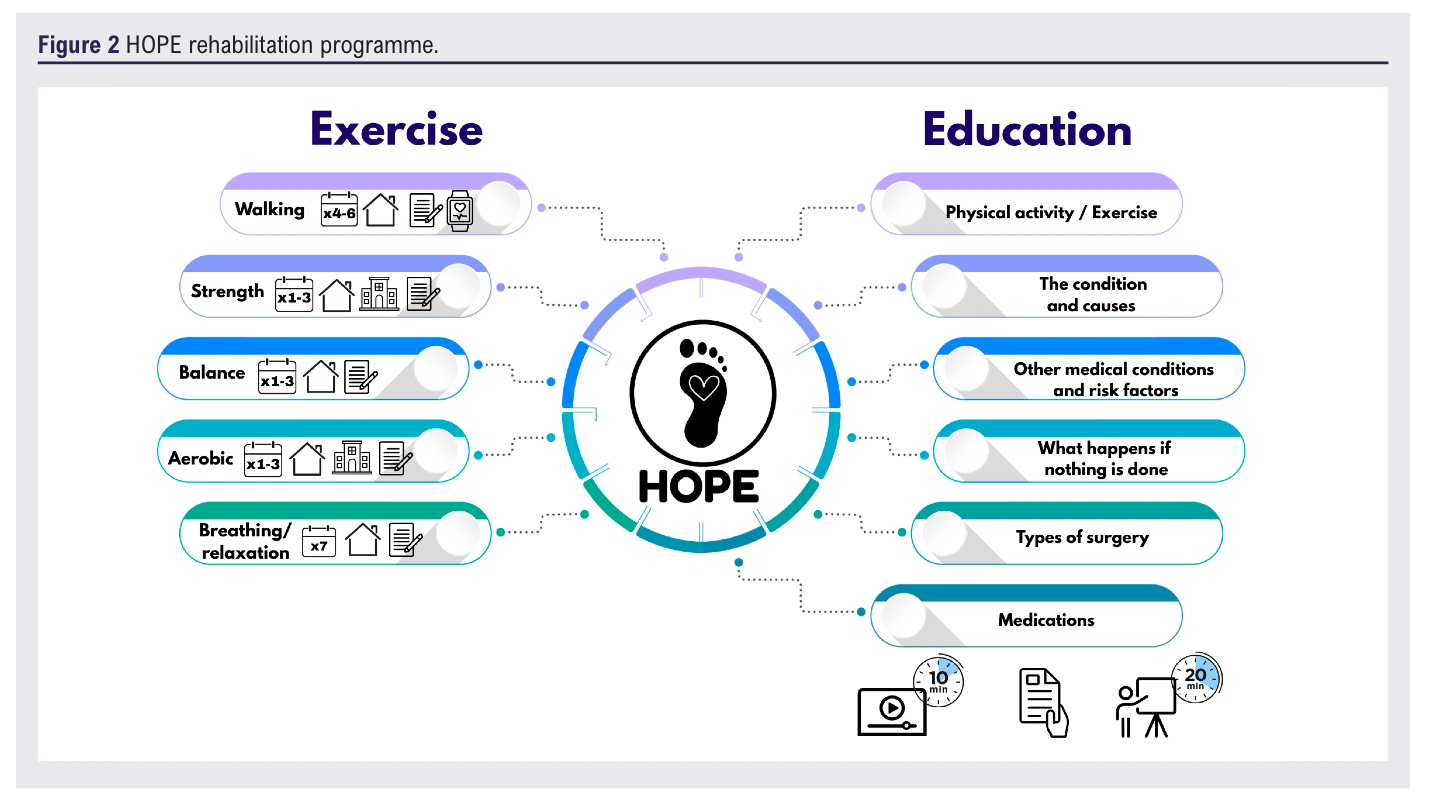
This exercise yielded a final dataset of 35 items which served as the foundation for the design and content of the rehabilitation programme. This dataset delineated the specific activities to be incorporated within the exercise component alongside recommendations regarding their frequency, setting and appropriate methods of monitoring. Additionally, the dataset informed the content to be addressed within the educational component of the programme, including guidance on optimal delivery methods and scheduling (Figure 2).
These findings are consistent with several clinical guidelines for individuals presenting with cardiovascular health conditions.33–36 All guidance underpins the therapeutic value of education, physical activity and structured exercise in improving functional capacity, symptom burden and quality of life, while also recognising the need for adaptable delivery models to address barriers to access and adherence.
While expert opinion sits at the lowest level of the evidence pyramid,37 the Delphi method is considered the most widely used consensus group technique for exploring emerging areas of uncertainty,38 due to the integration of anonymity, iterative rounds, structured feedback and statistical synthesis of group responses.39 A key strength of this study was the recruitment of a diverse range of international experts including healthcare professionals, individuals living with CLTI and carers. This inclusive approach facilitated the generation of domains that reflect a broad spectrum of perspectives rather than privileging insights from a single subgroup. An additional methodological strength was the geographical diversity of the participant pool, which enhanced the contextual richness and generalisability of the findings.
Across successive rounds, responses from both individuals with CLTI/carers and healthcare professionals demonstrated alignment regarding rehabilitation, education and exercise. A notable divergence, however, emerged in perceptions of patient knowledge. Whilst half of the individuals with CLTI/carers reported knowing ‘a lot’ about the condition, the majority of healthcare professionals perceived that patients knew ‘very little’. Although this aligns with other studies,40 this discrepancy may simply be due to differing interpretations of what it means to ‘know’ about CLTI – for example, individuals with CLTI may perceive themselves to be well informed based on lived experience whereas healthcare professionals may assess knowledge based on clinical accuracy or adherence to recommendations. Consistent with other studies,41,42 however, both groups agreed upon the provision of education within the rehabilitation programme.
Attrition rates are recognised as a limitation of the Delphi technique,16,43,44 with rates as high as 92% reported in some studies.45 This study yielded an attrition rate of 49% and 72% across successive rounds, reflecting the challenge of sustaining participant engagement. Although representation from both individuals with CLTI/carers and healthcare professionals was maintained throughout, the final workshop included significantly fewer patients/carers (n=3) than healthcare professionals (n=6), which may have influenced the findings. Although patients are often regarded as the most vulnerable and least empowered members of multidisciplinary teams,46 active and meaningful participation was observed during the workshop. This engagement was likely facilitated by thorough preparation, facilitator support and the creation of a safe and inclusive environment.47 Notably, response rates (a key indicator of the validity and reliability of survey-based research)48 remained robust, consistently exceeding the average reported rate for online surveys (44.1%).49
Research to date has primarily focused on supervised exercise therapy for intermittent claudication after revascularisation, and while recent protocols have begun to incorporate patients with CLTI into cardiac rehabilitation,18 this is, to our knowledge, the first bespoke rehabilitation programme developed exclusively for the post-revascularisation CLTI population. Whilst there is no formal guidance specific to the CLTI population, the European Society of Cardiology and global vascular guidelines certainly advocate exercise following revascularisation.5 However, this guidance is extremely vague due to the lack of research and data to validate it. This study has taken the initial step forward to address several of the top 10 research priorities as identified by a JLA and Vascular Society of Great Britain and Ireland priority setting partnership, including the number 1 priority: “What can be done to improve outcomes in patients with severe circulation problems to their legs?”
Conclusion
This study has captured the perspectives and opinions of experts, patients and carers to inform the design of a rehabilitation programme suitable for individuals with CLTI following revascularisation surgery.
The key components of the programme include a range of physical activities (aerobic, strength training and balance) to be carried out at home and in a supervised venue, all monitored via diary and an activity monitor. A range of educational topics were identified, all to be delivered via presentations and supported with information leaflets and online videos.
While the results align with current guidelines provided for those with similar clinical conditions, this is the first individualised rehabilitation programme specific to this population. This study has taken initial steps to address key research priorities and the next step is to conduct a multicentre feasibility trial in both community and NHS settings.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2026;ONLINE AHEAD OF PUBLICATION
Publication date:
February 23, 2026
Author Affiliations:
1. Department of Sport and Exercise Sciences, Manchester Metropolitan University, Institute of Sport, Manchester, UK
2. Department of Cardiovascular Sciences, University of Leicester, Leicester, UK
3. NIHR Leicester Biomedical Research Centre, BHF Cardiovascular Research Facility, Leicester, UK
4. Manchester Centre for Health Psychology, School of Medical Sciences, Faculty of Biology, Medicine and Health, University of Manchester, Manchester, UK
Corresponding author:
Mrs Joanne Duff
Department of Sport and
Exercise Sciences, Manchester Metropolitan University,
Institute of Sport, Manchester, M1 7EL, UK
Email: joanne.duff@ stu.mmu.ac.uk


")

")

