ORIGINAL RESEARCH
Embedding lived experience into the development of a rehabilitation programme for individuals with chronic limb-threatening ischaemia
Duff J,1 Saratzis A,2,3 Bartlett YK,4 Harwood AE,1 Haque A,5 Edwards H,1 Olsen N,6 Birkett S1
Plain English Summary
Why we undertook the work: Peripheral artery disease (PAD) affects millions of people worldwide and in its most severe form chronic limb-threatening ischaemia (CLTI) individuals face a number of health challenges. Although surgery can help restore blood flow to the leg/s, patients have highlighted the need for better education and additional support to live a healthier life. We therefore aimed to develop a programme that includes exercise and education to help them achieve this. Importantly, we wanted individuals with CLTI and their carers to help guide our research so that the programme reflects what matters most to patients.
What we did: We involved patients and their carers throughout our research project. Some helped with the study design and funding application, and others helped to prepare our questionnaires. Patients, carers and health professionals were invited to complete the questionnaires and attend an online workshop so they could share their views on exercise and education. Their responses helped identify the components that should be included in a rehabilitation programme. As part of the education aspect we created information sheets and presentations. Some patients and carers reviewed them and gave feedback. We also used the information in the questionnaires to understand what stops individuals from exercising and what we could put into place to help.
What we found: Involving patients and their carers helped shape our study in several ways. Their input improved the relevance and clarity of the study questions and ensured that the programme addressed real-world concerns. The questionnaires and workshop helped to identify the challenges that patients face after surgery and what is needed to support them. Patient feedback also helped improve the layout, language, images and overall clarity of the educational resources. However, as fewer people participated in this part of the research, it highlighted the importance of communicating with participants and offering different ways for them to provide feedback.
What this means: This work shows that involving people with lived experience of a condition can strengthen health research. By working together with patients and carers we were able to design a rehabilitation programme that is based on patient priorities and lived experience. The next step is to test the programme in a future study to see whether it is feasible and beneficial. Continued involvement of patients and their carers will remain central to this work.
Abstract
Background: Public and patient involvement and engagement (PPIE) is essential to improving the relevance, quality and impact of health research, while also offering potential benefits for those involved. Guided by the GRIPP-2 framework, this paper reports how PPIE was embedded throughout the development of a vascular rehabilitation programme for individuals with chronic limb-threatening ischaemia (CLTI) post revascularisation.
Method: Patient priorities identified in a James Lind Alliance (JLA) priority setting partnership initiated the study; individuals with lived experience supported the study design and funding application. A pre-study advisory group contributed to the protocol and development of the modified Delphi study. Alongside healthcare professionals, patients and carers participated in the Delphi activity which directly informed the structure and content of the rehabilitation intervention. Subsequent PPIE activity focused on refining educational materials and intervention components.
Results: Patient feedback improved accessibility, clarity and acceptability of programme resources, while behavioural barriers identified during the Delphi process informed the inclusion of structured behaviour-change tools.
Conclusion: Overall, embedding PPIE throughout strengthened the methodological rigour and applied relevance of the study. Continued commitment to meaningful PPIE will guide future feasibility testing of the rehabilitation programme.
Introduction
Public and patient involvement and engagement
There is increasing recognition that involving individuals with lived experience of a health condition in public and patient involvement and engagement (PPIE) activities enhances the overall quality of the research.1-3 Beyond strengthening the research itself, evidence suggests that patient participation may benefit the individual directly, by developing their skills and knowledge and increasing their self-confidence and self-satisfaction.4-6 Defining PPIE as research conducted with or by individuals with lived experience, rather than to, about or for them,7 and guided by the GRIPP-2 long form,8 this paper presents an overview of how the involvement of individuals with lived experience of peripheral artery disease (PAD) and their carers has been embedded throughout the research project, from priority setting through to the creation and refinement of a rehabilitation programme. In reporting this work, we aim to highlight the methodological importance and applied impact of integrating PPIE expertise in vascular rehabilitation research.
Peripheral artery disease
Peripheral artery disease (PAD) affects more than 236 million people globally, with prevalence continuing to rise.9 Its most severe form, chronic limb-threatening ischaemia (CLTI), affects around 11% of PAD patients,10 and is associated with poor mobility, frailty and reduced quality of life.11,12 Even after successful revascularisation, reported mortality rates approach 50% within one to three years, 42% of patients experience major adverse cardiovascular events (MACE) such as myocardial infarction and stroke, and major amputation occurs in up to 20% of cases within the same time frame.13-15 Whilst the benefits of a supervised exercise programme post revascularisation are established in those with the less severe manifestation of the disease (intermittent claudication),16 there is a notable absence of studies evaluating whether similar benefits are observed in those with CLTI post revascularisation.
Research priorities
Individuals who live with a medical condition are encouraged to participate in establishing research priorities,17 therefore priority setting partnerships (PSPs) such as those facilitated by the James Lind Alliance (JLA) bring patients and healthcare professionals together on an equal footing to identify evidence uncertainties and prioritise them.18 Recently 373 patients and carers helped to identify the top 10 research priorities for PAD.19 Three of them included: how can we reduce cardiovascular risk in PAD patients; how can we help educate better those patients who have poor circulation to their legs; and what can be done to improve outcomes in patients with severe circulation problems to their legs? In the absence of guidance specific to those with CLTI post revascularisation,20 we conducted a modified Delphi study to inform the development of a rehabilitation programme specifically for this population.21 This process represents an initial step toward addressing several of the identified research priorities and ensuring that subsequent programme development is firmly grounded in patient identified needs and priorities (Figure 1). The subsequent stages in the research project will involve a feasibility study to assess the acceptability and practicality of the intervention, followed by (if progression criteria are achieved) a randomised controlled trial to evaluate its effectiveness.
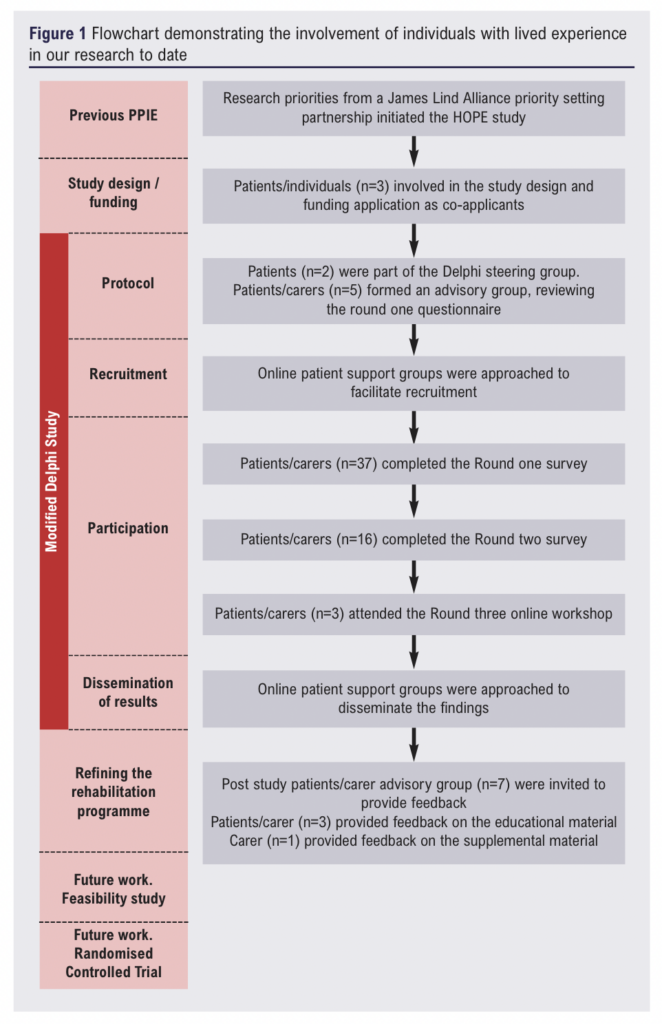
Study protocols and funding application
PPIE was embedded from the earliest stages of the research cycle, with three PPIE co-applicants contributing to a National Institute for Health and Care Research (NIHR) Research for Patient Benefit (RfPB) funding application, and development of the Delphi study and feasibility study protocols. The first co-applicant who lives with CLTI has completed training modules provided by the NIHR, has represented patient perspectives across multiple PPIE focus groups, and has involvement in several research studies as a patient participant. The second, who is a double amputee as a consequence of CLTI, has participated in two previous research studies as a patient. The third, who is a health and wellbeing professional, actively works within minoritised ethnic communities. All three reviewed the study protocols and the lay summaries to ensure equality, diversity and inclusivity. Suggestions included provision of a chaperone, a translation service, and changing the word “arteries” in the lay summary to “blood vessels”. All contributors were treated in accordance with ethical research principles,22 and will receive funding for their time and commitment in accordance to the NIHR. All three were invited to join the modified Delphi study steering group. Whilst formal training was not provided, ongoing communication from the research team was offered throughout to facilitate meaningful engagement.
Modified Delphi study
Delphi is a consensus-driven technique, widely adopted in health services research, to harness the insights of healthcare professionals and individuals with lived experience of health conditions.23 The purpose of this report is to describe how PPIE was embedded throughout our work. The full methodology and findings can be found in the published study.21
Steering group and advisory group
The research team brings together expertise spanning health psychology, clinical exercise physiology, cardiovascular rehabilitation and vascular surgery. Collectively, the team has extensive experience in the co-design, delivery and evaluation of complex rehabilitation interventions using mixed-methods and consensus-based approaches, including Delphi studies that integrate patient and clinician perspectives. Following the death of one of the PPIE contributors as a result of their condition, two of the three contributors joined the research team to form a steering group and coordinate the study activity. Additionally, alongside two other individuals with CLTI and a carer of an individual with CLTI (n=5), an advisory group was formed. As initial data for Delphi studies are collected via participant questionnaires, the advisory group reviewed the patient/carer questionnaire that had been designed by the research team. It was important to ensure that the questions pertaining to rehabilitation, exercise and educational needs were understandable, meaningful and aligned with patient priorities. Responses from the group included “maybe reword, have you/the person with CLTI had surgery?”, “include some examples (of rehabilitation)” and “add the question, do you think it is necessary? (rehabilitation)” The feedback led to several refinements, including rewording items, additional questions, and the inclusion of illustrative examples to improve clarity and relevance.
Recruitment and participation
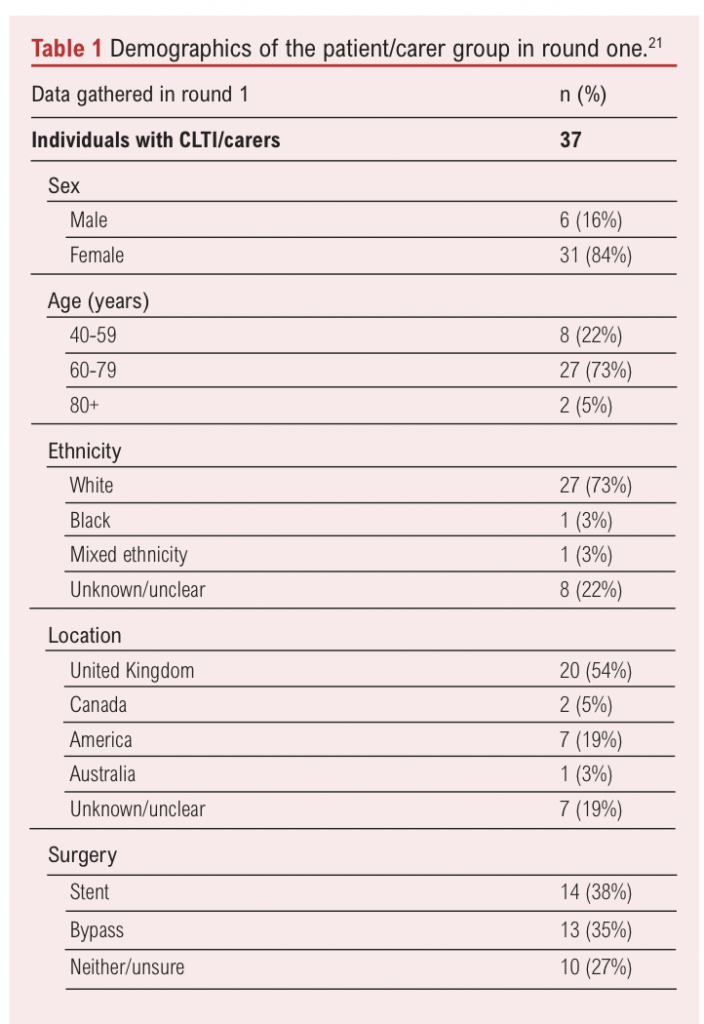
The study took place from November 2024 until June 2025. As social media provide an effective platform for connecting and engaging with patients within a condition- specific population,24,25 patient and carer participants were recruited through patient- and public-led PAD Facebook groups. A member of the research team engaged with patients and carers via a webinar hosted by the Global PAD Association to support participation. In the initial round of the modified Delphi study, 20 healthcare professionals and 37 patients/carers responded to open-ended questions pertaining to rehabilitation, exercise and education. Demographics of the patient/carer group collected in round one are provided in Table 1.
In the second-round questionnaire 13 healthcare professionals and 16 patients/carers evaluated the inclusion of items that had been identified in round one, by indicating their level of agreement. Consensus was pre-defined as >70% agreement. The final round ran as an online workshop, attended by six healthcare professionals and three patients/carers. All findings were presented to participants, and topics that had not achieved consensus were subjected to further review, discussion and re-evaluation through a voting process. The modified Delphi process successfully produced a final data set that informed the structure and content of the rehabilitation programme (Figure 2).

Reporting and dissemination of results
The Delphi study was reported in accordance with CREDES guidance,26 and the GRIPP-2 short form was utilised, as both ensure thorough and transparent reporting of PPIE throughout the process.7,27
In addition to publication in a peer-reviewed journal,21 and presentation at a scientific conference, the results were disseminated via the patient- and public-led Facebook groups that facilitated study recruitment. Evidence suggests that sharing the findings with the community that contributed to the initial stages of the research reinforces trust, demonstrates the impact of involvement and helps to sustain ongoing engagement in research activities.28
Refining the rehabilitation programme after the Delphi study
The Delphi activity established that the rehabilitation programme post revascularisation should include education on the condition and its causes, physical activity and exercise, other medical conditions and risk factors, what happens if nothing is done, types of surgery, and medications. Written educational material is only effective if it can be read, understood and remembered,29 so patients with lived experience are ideally positioned to assess the comprehensibility, acceptability and actionability of such material.30 Therefore, during the Delphi study participants were invited to indicate their interest in contributing to the development of the educational material (PowerPoint presentations and information sheets) which would take place after the Delphi activity itself. Once the material had been created by the research team it was emailed to the seven patients and carers who had expressed interest. Three contributors responded, offering comments such as “the educational material contains too much information and is crowded” and “some images are a bit drab,” alongside suggestions including “images could be a bit brighter” and “font size could be bigger.” The feedback received led to refinement of the layout, imagery, content and tone. The revised material was emailed back to the contributors and one responded, commenting “this material is far better presented”, “the layout is somewhat more understandable” and “the pictures are far more relatable”.
Adhering to clinical recommendations such as increasing physical activity is often challenging, as many find it difficult to adopt and maintain changes.31 Therefore barriers to exercise that had been reported by participants during the Delphi process were categorised by members of the research team using the COM-B model (Capability Opportunity Motivation – Behaviour).32 This helped the research team to understand what would need to change for the behaviour (exercising) to take place, and furthermore facilitated identification of potential interventions that might support this change.32 Mapping barriers such as the weather (opportunity), co-morbidities (capability) and mental health (motivation) directly informed refinement of the programme. This included the incorporation of volitional help sheets33 and action planning tools,34 which participants can utilise in conjunction with the educational sessions. Seven patient/carers were invited to provide feedback and one responded, expressing strong advocation for the additional resources.
Reflection and future research
Via mixed methods, PPIE meaningfully influenced multiple stages of the research cycle, with the most substantial impact occurring during the Delphi exercise itself. This was attributed to context and process factors such as targeting a specific audience and disseminating the questionnaires online. Attrition rates are recognised as a limitation of the Delphi technique;35 whilst attrition was high across successive rounds, representation from both individuals with CLTI/carers and healthcare professionals was maintained throughout. The final workshop included significantly fewer patients/carers (n=3) than healthcare professionals (n=6) which may have influenced the findings. However, throughout the workshop we experienced effective and meaningful patient participation. Notably, a patient contributor highlighted that although information on physical activity and exercise would be referenced within the broader category of risk factors, its significance warranted recognition as a separate topic. This prompted further group discussion and a unanimous decision to include it as a standalone topic. Evidence suggests that active patient participation is due to adequate preparation, facilitator guidance and a trusting, supportive atmosphere.36 We achieved this through the advanced distribution of workshop invitations, providing detailed information regarding the workshop content and schedule, and by following up with reminder emails. During the workshop, all facilitators introduced themselves and emphasised that all contributions were valued and considered important.
Feedback from those with lived experience strengthens confidence in the perceived need and acceptability of the educational material, but engagement during our refinement stage was poor. This highlights the importance of investing in relationships and support mechanisms to ensure long-term and meaningful participation. Whilst there is no evidence that alternative methods such as interviews and focus groups would have encouraged additional participants to provide feedback on the educational material,37 offering multiple channels for feedback such as anonymous submission might have done.38 Furthermore, as low participation rates are often due to uncertainty about what is required, or feeling overburdened by what is expected,39 we will provide additional support, clearer guidance and flexible feedback options to encourage participation in future.
Conclusion
To enhance the quality of healthcare research it is essential to involve those who have lived experience of the health condition being researched. Involving individuals with lived experience of PAD and CLTI has proved valuable in the context of our study conception, design, recruitment, insights, dissemination and refinement of the intervention, and the research team remains committed to harness the insights of patients and carers as the project progresses. To strengthen relationships with patient and carer contributors in the forthcoming feasibility trial additional support and improved communication pathways will be implemented, including regular updates, clear guidance on tasks and additional channels for feedback. These measures aim to enable deeper and sustained engagement and ensure that those with lived experience continue to shape the research process.
Article DOI:
Journal Reference:
J.Vasc.Soc.G.B.Irel. 2026;5(3):145-151
Publication date:
May 27, 2026
Author Affiliations:
1. Department of Sport and Exercise Sciences, Manchester Metropolitan University, Institute of Sport, Manchester, UK
2. Department of Cardiovascular Sciences, University of Leicester, Leicester, UK
3. NIHR Leicester Biomedical Research Centre, BHF Cardiovascular Research Facility, Leicester, UK
4. Manchester Centre for Health Psychology, School of Medical Sciences, Faculty of Biology, Medicine and Health, University of Manchester, Manchester, UK
5. Cardiovascular Sciences, School of Medical Sciences, Faculty of Biology, Medicine and Health, University of Manchester, UK
6. Patient representative, HOPE Advisory Group, UK
Corresponding author:
Mrs Joanne Duff Department of Sport and
Exercise Sciences, Manchester Metropolitan University, Institute of Sport, Manchester, M1 7EL, UK
Email: joanne.duff@ stu.mmu.ac.uk


")

")

